

Stroke-induced activation of the α7 nicotinic receptor increases Pseudomonas aeruginosa lung injury
- PMID: 22490926
- PMCID: PMC3382094
- DOI: 10.1096/fj.11-197384
Stroke-induced activation of the α7 nicotinic receptor increases Pseudomonas aeruginosa lung injury
Abstract
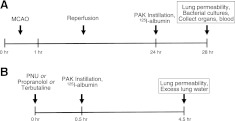
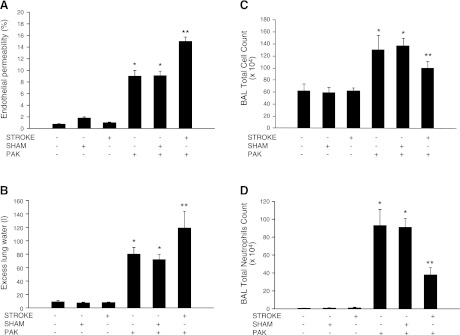
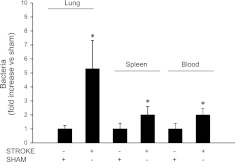
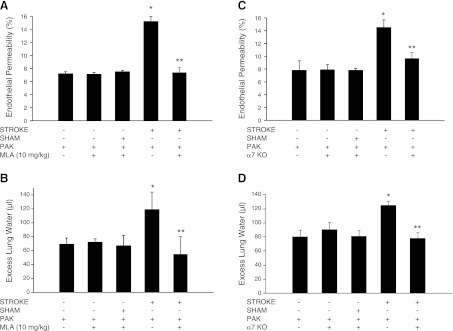
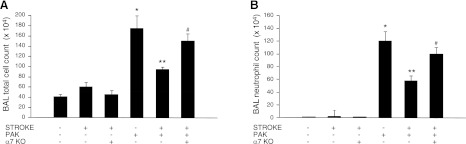
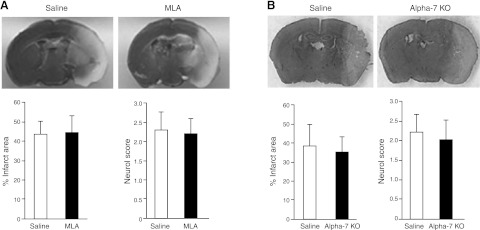
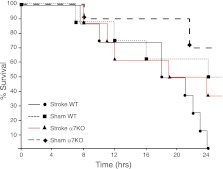
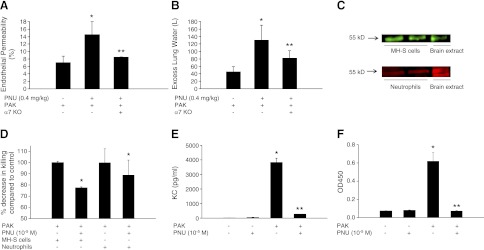
Infectious complications, predominantly pneumonia, are the most common cause of death in the postacute phase of stroke, although the mechanisms underlying the corresponding immunosuppression are not fully understood. We tested the hypothesis that activation of the α7 nicotinic acetylcholine receptor (α7nAChR) pathway is important in the stroke-induced increase in lung injury caused by Pseudomonas aeruginosa pneumonia in mice. Prior stroke increased lung vascular permeability caused by P. aeruginosa pneumonia and was associated with decreased lung neutrophil recruitment and bacterial clearance in mice. Pharmacologic inhibition (methyllycaconitine IC(50): 0.2-0.6 nM) or genetic deletion of the α7nAChR significantly (P<0.05) attenuates the effect of prior stroke on lung injury and mortality caused by P. aeruginosa pneumonia in mice. Finally, pretreatment with PNU-282987, a pharmacologic activator of the α7nAChR (EC(50): 0.2 μM), significantly (P<0.05) increased lung injury caused by P. aeruginosa pneumonia, significantly (P<0.05) decreased the release of KC, a major neutrophil chemokine, and significantly (P<0.05) decreased intracellular bacterial killing by a mouse alveolar macrophage cell line and primary mouse neutrophils. In summary, the α7 nicotinic cholinergic pathway plays an important role in mediating the systemic immunosuppression observed after stroke and directly contributes to more severe lung damage induced by P. aeruginosa.
Figures

References
-
- Rothwell P. M., Algra A., Amarenco P. (2011) Medical treatment in acute and long-term secondary prevention after transient ischaemic attack and ischaemic stroke. Lancet 377, 1681–1692 - PubMed
-
- Henon H., Godefroy O., Leys D., Mounier-Vehier F., Lucas C., Rondepierre P., Duhamel A., Pruvo J. P. (1995) Early predictors of death and disability after acute cerebral ischemic event. Stroke 26, 392–398 - PubMed
-
- Kalra L., Yu G., Wilson K., Roots P. (1995) Medical complications during stroke rehabilitation. Stroke 26, 990–994 - PubMed
-
- Langhorne P., Stott D. J., Robertson L., MacDonald J., Jones L., McAlpine C., Dick F., Taylor G. S., Murray G. (2000) Medical complications after stroke: a multicenter study. Stroke 31, 1223–1229 - PubMed
-
- Hilker R., Poetter C., Findeisen N., Sobesky J., Jacobs A., Neveling M., Heiss W. D. (2003) Nosocomial pneumonia after acute stroke: implications for neurological intensive care medicine. Stroke 34, 975–981 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
