

Evaluation of deformable image registration and a motion model in CT images with limited features
- PMID: 22491010
- PMCID: PMC3349335
- DOI: 10.1088/0031-9155/57/9/2539
Evaluation of deformable image registration and a motion model in CT images with limited features
Abstract
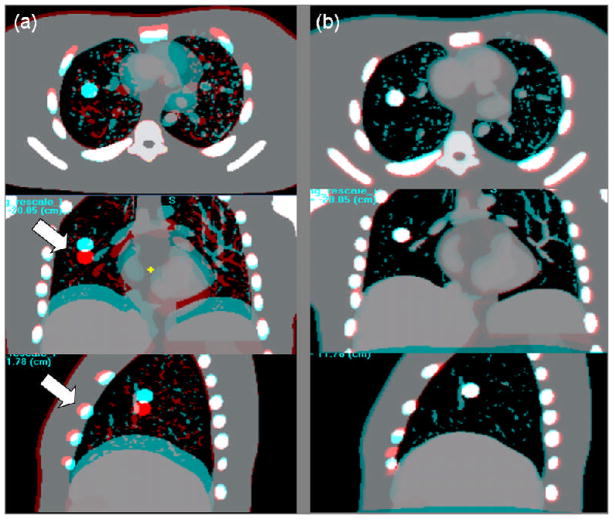
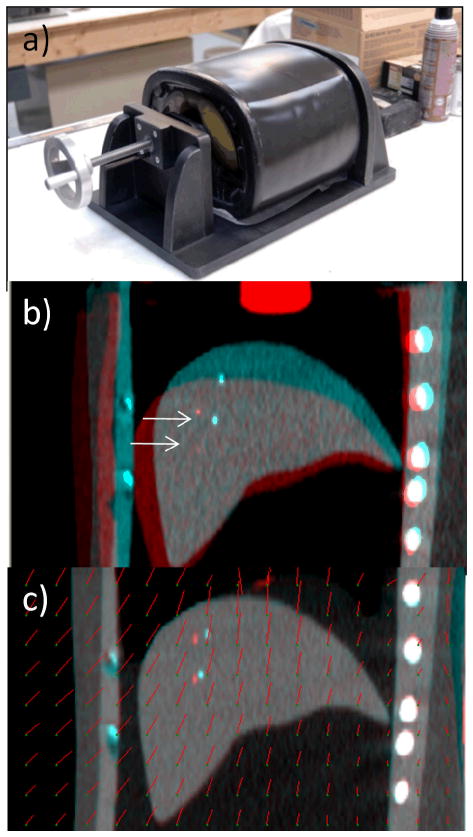
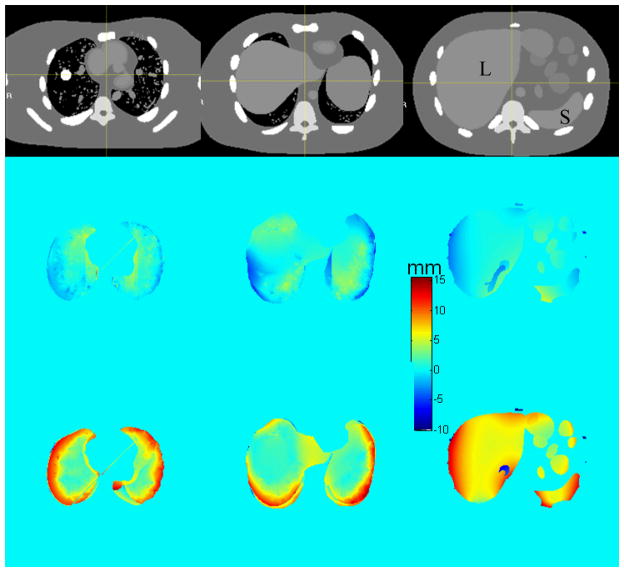
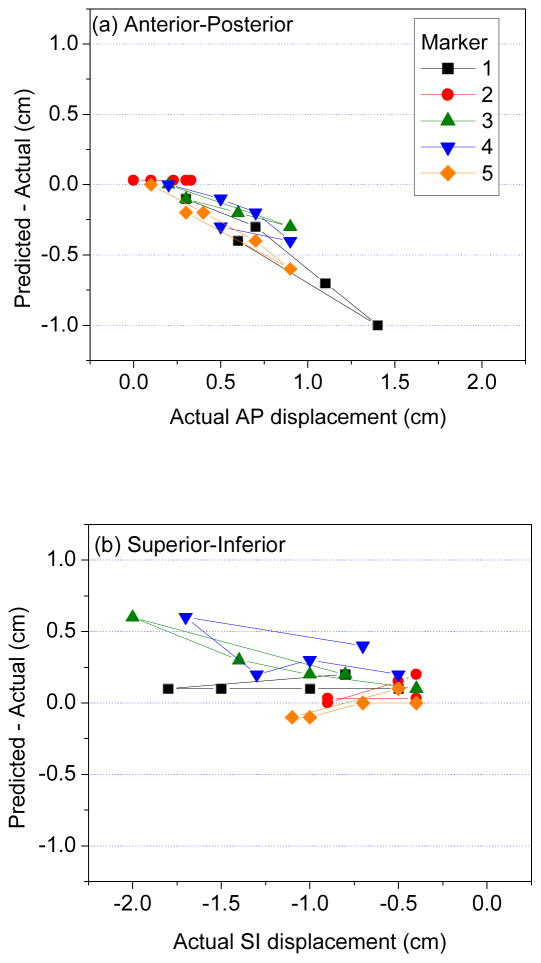
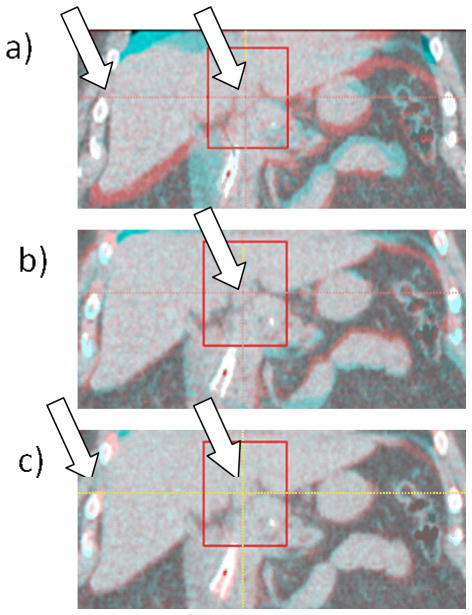
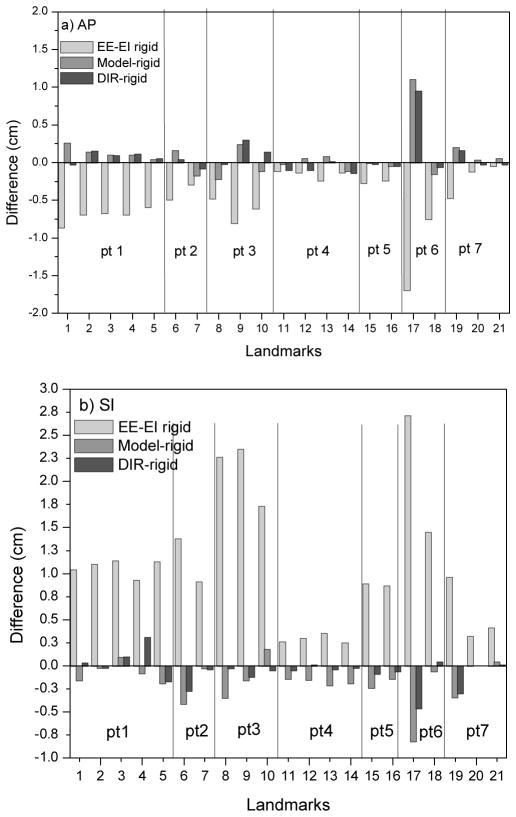
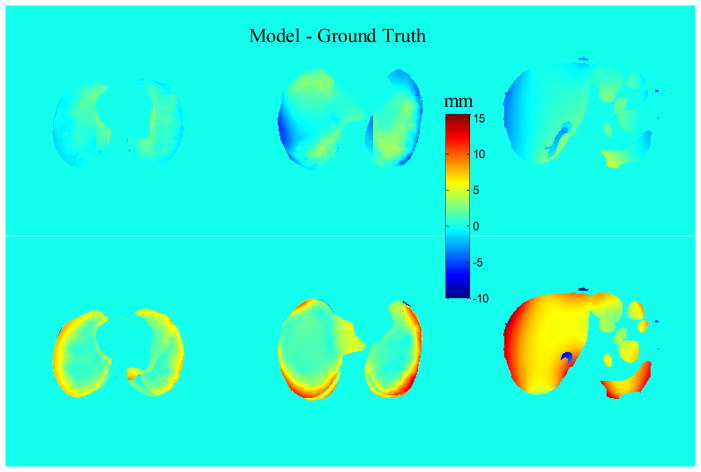
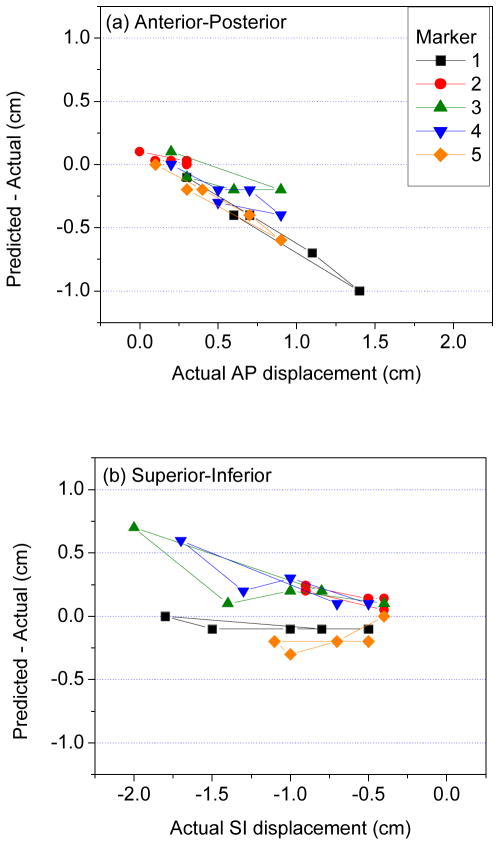
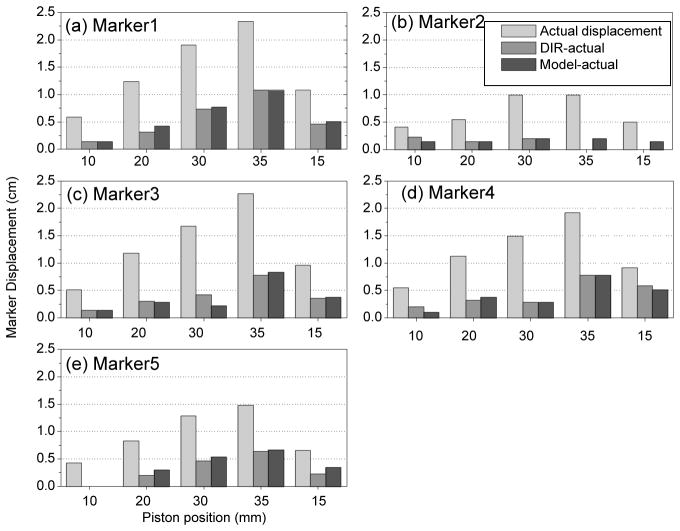
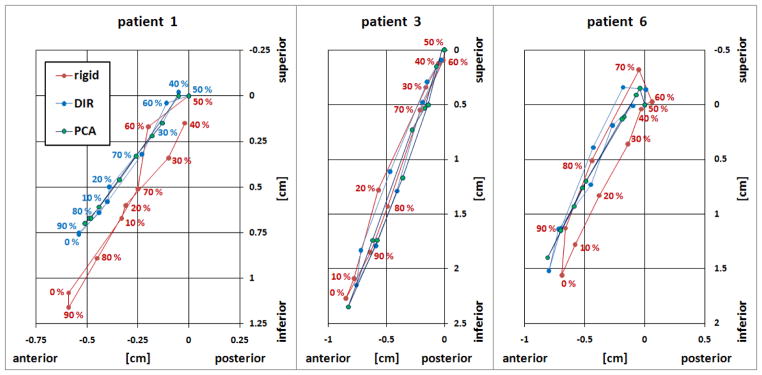
Deformable image registration (DIR) is increasingly used in radiotherapy applications and provides the basis for a previously described model of patient-specific respiratory motion. We examine the accuracy of a DIR algorithm and a motion model with respiration-correlated CT (RCCT) images of software phantom with known displacement fields, physical deformable abdominal phantom with implanted fiducials in the liver and small liver structures in patient images. The motion model is derived from a principal component analysis that relates volumetric deformations with the motion of the diaphragm or fiducials in the RCCT. Patient data analysis compares DIR with rigid registration as ground truth: the mean ± standard deviation 3D discrepancy of liver structure centroid positions is 2.0 ± 2.2 mm. DIR discrepancy in the software phantom is 3.8 ± 2.0 mm in lung and 3.7 ± 1.8 mm in abdomen; discrepancies near the chest wall are larger than indicated by image feature matching. Marker's 3D discrepancy in the physical phantom is 3.6 ± 2.8 mm. The results indicate that visible features in the images are important for guiding the DIR algorithm. Motion model accuracy is comparable to DIR, indicating that two principal components are sufficient to describe DIR-derived deformation in these datasets.
Figures
References
-
- Keall P. 4-dimensional computed tomography imaging and treatment planning. Semin Radiat Oncol. 2004;14:81–90. - PubMed
-
- Dieterich S, Cleary K, D’Souza W, Murphy MJ, Wong KH, Keall P. Locating and targeting moving tumors with radiation beams. Med Phys. 2008;35 (12):5684– 5694. - PubMed
-
- Yan D, Jaffray DA, Wong JW. A model to accumulate fractionated dose in a deforming organ. Int J Radiat Oncol Biol Phys. 1999;44:665–675. - PubMed
-
- Wu C, Jeraj R, Olivera GH, Mackie TR. Re-optimization in adaptive radiotherapy. Phys Med Biol. 2002;47:3181–3195. - PubMed
-
- Birkner M, Yan D, Alber M, et al. Adapting inverse planning to patient and organ geometrical variation: algorithm and implementation. Med Phys. 2003;30:2822–2831. - PubMed