

Ten-year risk of diagnostic mammograms and invasive breast procedures after breast-conserving surgery for DCIS
- PMID: 22491230
- PMCID: PMC3328423
- DOI: 10.1093/jnci/djs167
Ten-year risk of diagnostic mammograms and invasive breast procedures after breast-conserving surgery for DCIS
Abstract
Background: Breast-conserving surgery (BCS) is the most common treatment for ductal carcinoma in situ (DCIS); however, how often women experience subsequent diagnostic evaluations over time is not known.
Methods: We identified 2948 women with DCIS who were treated with BCS from 1990 to 2001 and followed for up to 10 years at three integrated health-care delivery systems. We calculated the percentages of diagnostic mammograms and ipsilateral invasive procedures following the initial breast excision to treat DCIS, estimated the 10-year cumulative incidence of these procedures, and determined hazard ratios for both types of procedures with Cox regression modeling. All statistical tests were two-sided.
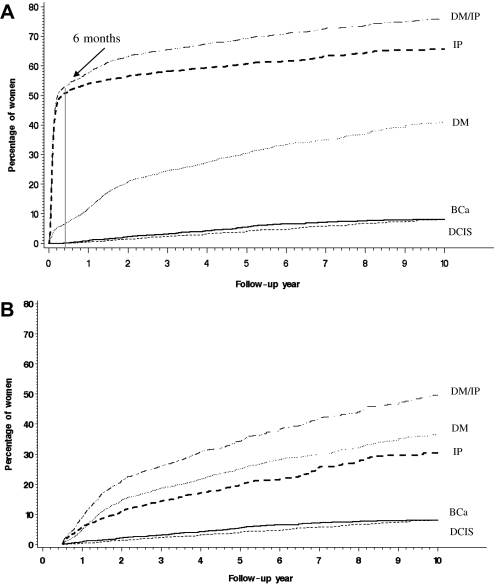
Results: Over 10 years, 907 women (30.8%) had 1422 diagnostic mammograms and 1813 (61.5%) had 2305 ipsilateral invasive procedures. Diagnostic mammograms occurred in 7.3% of women in the first 6 months and continued at a median annual rate of 4.3%. Ipsilateral invasive procedures occurred in 51.5% of women in the first 6 months and continued at a median annual rate of 3.1%. The estimated 10-year cumulative risk of having at least one diagnostic mammogram after initial DCIS excision was 41.0% (95% confidence interval [CI] = 38.5% to 43.5%); at least one invasive procedure, 65.7% (95% CI = 63.7% to 67.8%); and either event, 76.1% (95% CI = 74.1% to 78.1%). Excluding events in the first 6 months following initial DCIS excision, corresponding risks were 36.4% (95% CI = 33.8% to 39.0%) for diagnostic mammograms, 30.4% (95% CI = 26.9% to 33.8%) for invasive procedures, and 49.5% (95% CI = 45.6% to 53.5%) for either event.
Conclusions: Women with DCIS treated with BCS continue to have diagnostic and invasive breast procedures in the conserved breast over an extended period. The frequency of ongoing diagnostic breast evaluations should be included in discussions about treatment.
Figures
Comment in
-
Ductal carcinoma in situ (DCIS): raising signposts on an ill-marked treatment path.J Natl Cancer Inst. 2012 Apr 18;104(8):569-71. doi: 10.1093/jnci/djs184. Epub 2012 Apr 5. J Natl Cancer Inst. 2012. PMID: 22491227 No abstract available.
References
-
- Fisher B, Costantino J, Redmond C, et al. Lumpectomy compared with lumpectomy and radiation therapy for the treatment of intraductal breast cancer. N Engl J Med. 1993;328(22):1581–1586. - PubMed
-
- Fisher B, Dignam J, Wolmark N, et al. Tamoxifen in treatment of intraductal breast cancer: National Surgical Adjuvant Breast and Bowel Project B-24 randomised controlled trial. Lancet. 1999;353(9169):1993–2000. - PubMed
-
- Fisher B, Dignam J, Wolmark N, et al. Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: findings from the National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol. 1998;16(2):441–452. - PubMed
-
- Baxter NN, Virnig BA, Durham SB, Tuttle TM. Trends in the treatment of ductal carcinoma in situ of the breast. J Natl Cancer Inst. 2004;96(6):443–448. - PubMed
-
- Curran D, van Dongen JP, Aaronson NK, et al. Quality of life of early-stage breast cancer patients treated with radical mastectomy or breast-conserving procedures: results of EORTC Trial 10801. The European Organization for Research and Treatment of Cancer (EORTC), Breast Cancer Co-operative Group (BCCG) Eur J Cancer. 1998;34(3):307–314. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
