

Neural mechanisms underlying deafferentation pain: a hypothesis from a neuroimaging perspective
- PMID: 22491886
- PMCID: PMC3359448
- DOI: 10.1007/s00776-012-0209-9
Neural mechanisms underlying deafferentation pain: a hypothesis from a neuroimaging perspective
Abstract
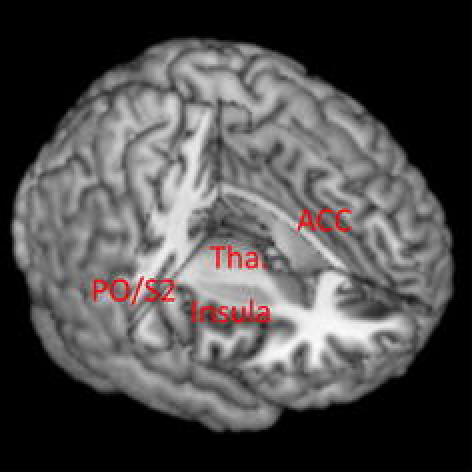
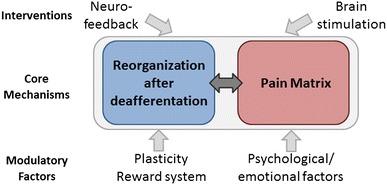
Deafferentation pain following nerve injury annoys patients, and its management is a challenge in clinical practice. Although the mechanisms underlying deafferentation pain remain poorly understood, progress in the development of multidimensional neuroimaging techniques is casting some light on these issues. Deafferentation pain likely results from reorganization of the nervous system after nerve injury via processes that interact with the substrates for pain perception (the pain matrix). Therapeutic effects of motor cortex stimulation on deafferentation pain suggest that the core mechanisms underlying deafferentation pain also interact with the motor system. Therefore, simultaneous neuroimaging and brain stimulation, an emerging neuroimaging technique, was developed to investigate complicated interactions among motor, somatosensory, and pain systems. In healthy participants, parts of the pain matrix (the anterior cingulate cortex, parietal operculum, and thalamus) show activity during both somatosensory stimulation and brain stimulation to the motor cortex. This finding indicates that motor, somatosensory, and pain systems communicate among each other via the neural network. A better understanding of the plastic mechanisms influencing such cross-talk among these systems will help develop therapeutic interventions using brain stimulation and neurofeedback.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
