

Lung protective mechanical ventilation and two year survival in patients with acute lung injury: prospective cohort study
- PMID: 22491953
- PMCID: PMC3320566
- DOI: 10.1136/bmj.e2124
Lung protective mechanical ventilation and two year survival in patients with acute lung injury: prospective cohort study
Abstract
Objective: To evaluate the association of volume limited and pressure limited (lung protective) mechanical ventilation with two year survival in patients with acute lung injury.
Design: Prospective cohort study.
Setting: 13 intensive care units at four hospitals in Baltimore, Maryland, USA.
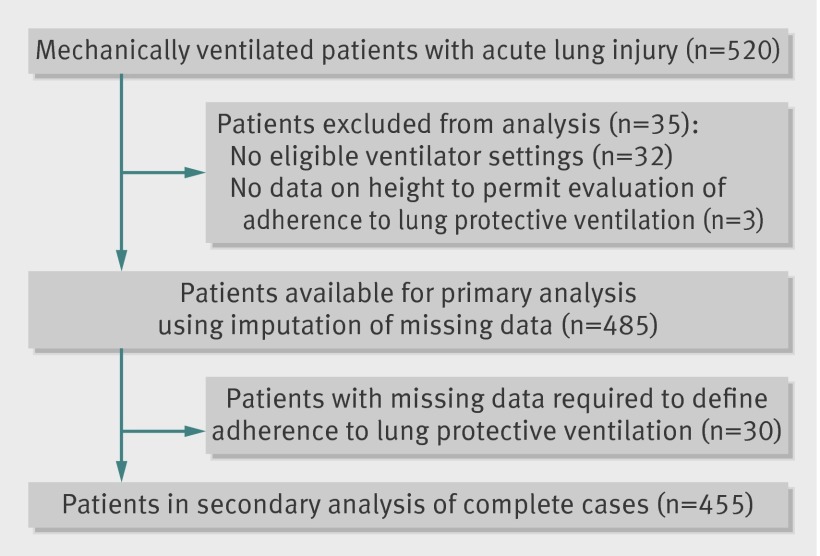
Participants: 485 consecutive mechanically ventilated patients with acute lung injury.
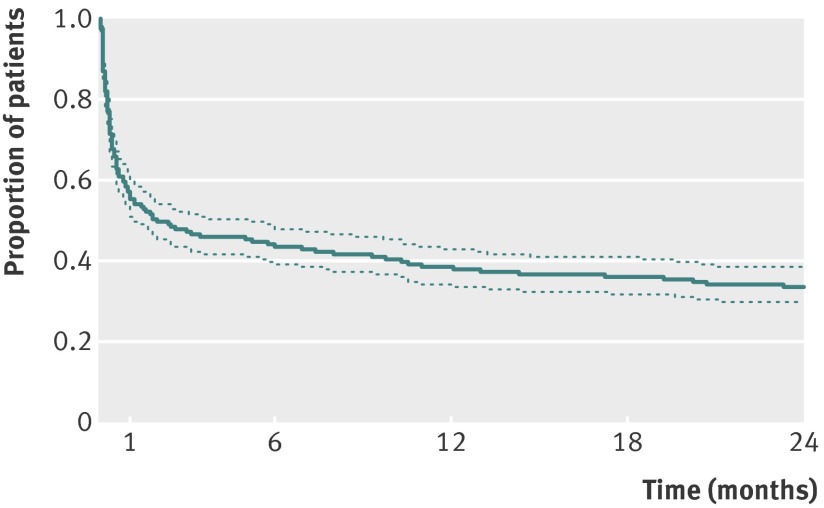
Main outcome measure: Two year survival after onset of acute lung injury.
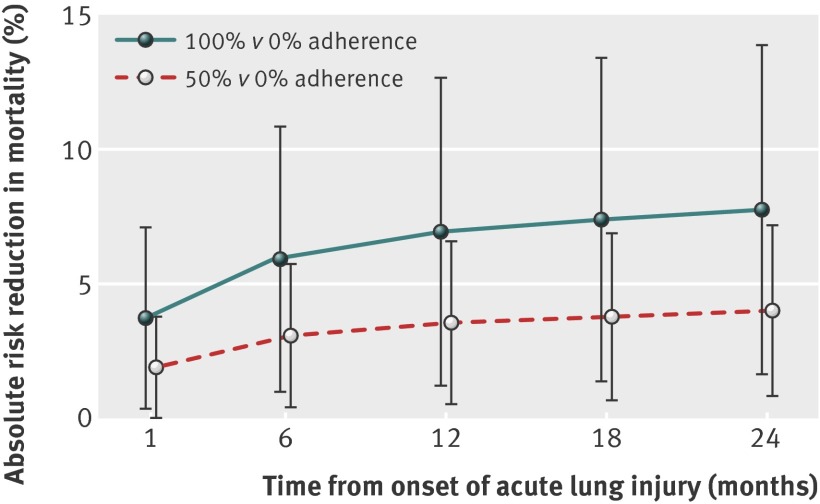
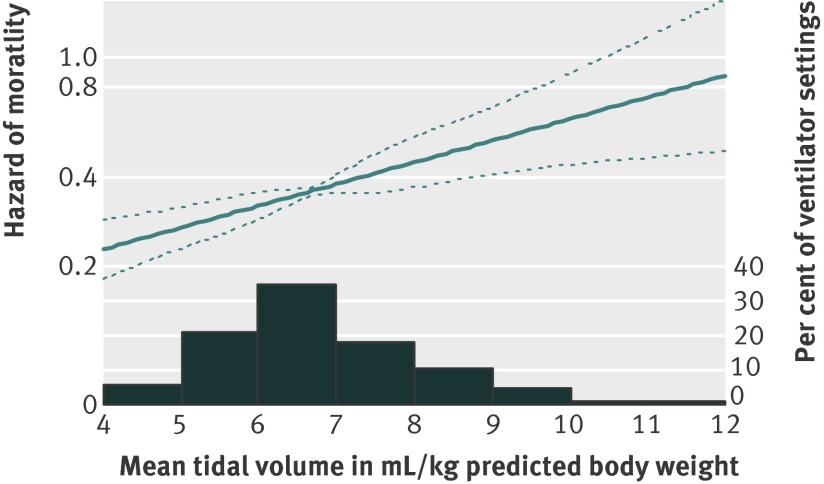
Results: 485 patients contributed data for 6240 eligible ventilator settings, as measured twice daily (median of eight eligible ventilator settings per patient; 41% of which adhered to lung protective ventilation). Of these patients, 311 (64%) died within two years. After adjusting for the total duration of ventilation and other relevant covariates, each additional ventilator setting adherent to lung protective ventilation was associated with a 3% decrease in the risk of mortality over two years (hazard ratio 0.97, 95% confidence interval 0.95 to 0.99, P=0.002). Compared with no adherence, the estimated absolute risk reduction in two year mortality for a prototypical patient with 50% adherence to lung protective ventilation was 4.0% (0.8% to 7.2%, P=0.012) and with 100% adherence was 7.8% (1.6% to 14.0%, P=0.011).
Conclusions: Lung protective mechanical ventilation was associated with a substantial long term survival benefit for patients with acute lung injury. Greater use of lung protective ventilation in routine clinical practice could reduce long term mortality in patients with acute lung injury.
Trial registration: Clinicaltrials.gov NCT00300248.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Lung protective ventilation.BMJ. 2012 Apr 5;344:e2491. doi: 10.1136/bmj.e2491. BMJ. 2012. PMID: 22491956 No abstract available.
References
-
- Herridge MS, Cheung AM, Tansey CM, Matte-Martyn A, Diaz-Granados N, Al Saidi F, et al. One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med 2003;348:683-93. - PubMed
-
- Desai SV, Law TJ, Needham DM. Long-term complications of critical care. Crit Care Med 2011;39:371-9. - PubMed
-
- Rubenfeld GD. Improving clinical trials of long-term outcomes. Crit Care Med 2009;37(Suppl ):S112-6. - PubMed
-
- Petrucci N, Iacovelli W. Lung protective ventilation strategy for the acute respiratory distress syndrome. Cochrane Database Syst Rev 2007;(3):CD003844. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical