

Exploring the cost-utility of stratified primary care management for low back pain compared with current best practice within risk-defined subgroups
- PMID: 22492783
- PMCID: PMC3465856
- DOI: 10.1136/annrheumdis-2011-200731
Exploring the cost-utility of stratified primary care management for low back pain compared with current best practice within risk-defined subgroups
Abstract
Objectives: Stratified management for low back pain according to patients' prognosis and matched care pathways has been shown to be an effective treatment approach in primary care. The aim of this within-trial study was to determine the economic implications of providing such an intervention, compared with non-stratified current best practice, within specific risk-defined subgroups (low-risk, medium-risk and high-risk).
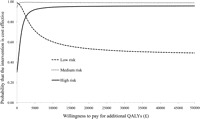
Methods: Within a cost-utility framework, the base-case analysis estimated the incremental healthcare cost per additional quality-adjusted life year (QALY), using the EQ-5D to generate QALYs, for each risk-defined subgroup. Uncertainty was explored with cost-utility planes and acceptability curves. Sensitivity analyses were performed to consider alternative costing methodologies, including the assessment of societal loss relating to work absence and the incorporation of generic (ie, non-back pain) healthcare utilisation.
Results: The stratified management approach was a cost-effective treatment strategy compared with current best practice within each risk-defined subgroup, exhibiting dominance (greater benefit and lower costs) for medium-risk patients and acceptable incremental cost to utility ratios for low-risk and high-risk patients. The likelihood that stratified care provides a cost-effective use of resources exceeds 90% at willingness-to-pay thresholds of £4000 (≈ 4500; $6500) per additional QALY for the medium-risk and high-risk groups. Patients receiving stratified care also reported fewer back pain-related days off work in all three subgroups.
Conclusions: Compared with current best practice, stratified primary care management for low back pain provides a highly cost-effective use of resources across all risk-defined subgroups.
Conflict of interest statement
Figures

References
-
- Maniadakis N, Gray A. The economic burden of back pain in the UK. Pain 2000;84:95–103 - PubMed
-
- Buchbinder R, Pransky G, Hayden J. Recent advances in the evaluation and management of nonspecific low back pain and related disorders. Best Pract Res Clin Rheumatol 2010;24:147–53 - PubMed
-
- Costa-Black KM, Loisel P, Anema JR, et al. Back pain and work. Best Pract Res Clin Rheumatol 2010;24:227–40 - PubMed
-
- Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J 2008;8:8–20 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
