

Interplay among BRAF, p16, p53, and MIB1 in pediatric low-grade gliomas
- PMID: 22492957
- PMCID: PMC3367847
- DOI: 10.1093/neuonc/nos077
Interplay among BRAF, p16, p53, and MIB1 in pediatric low-grade gliomas
Abstract
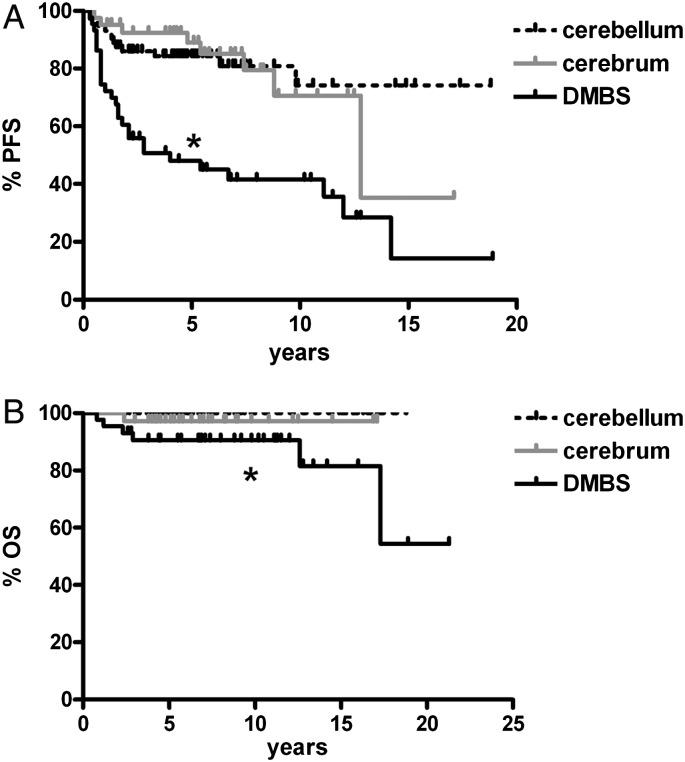
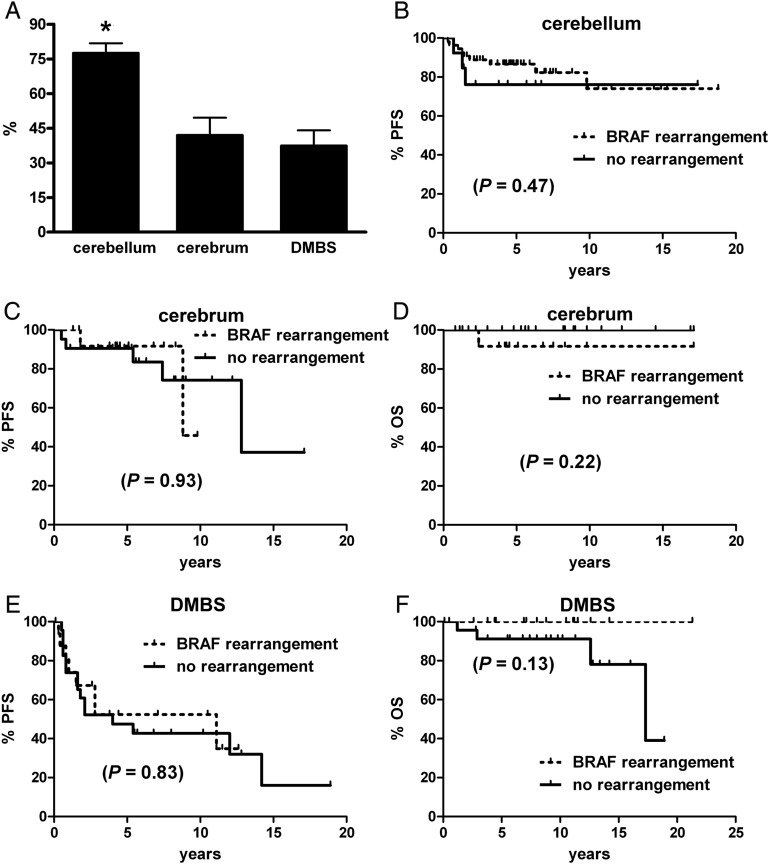
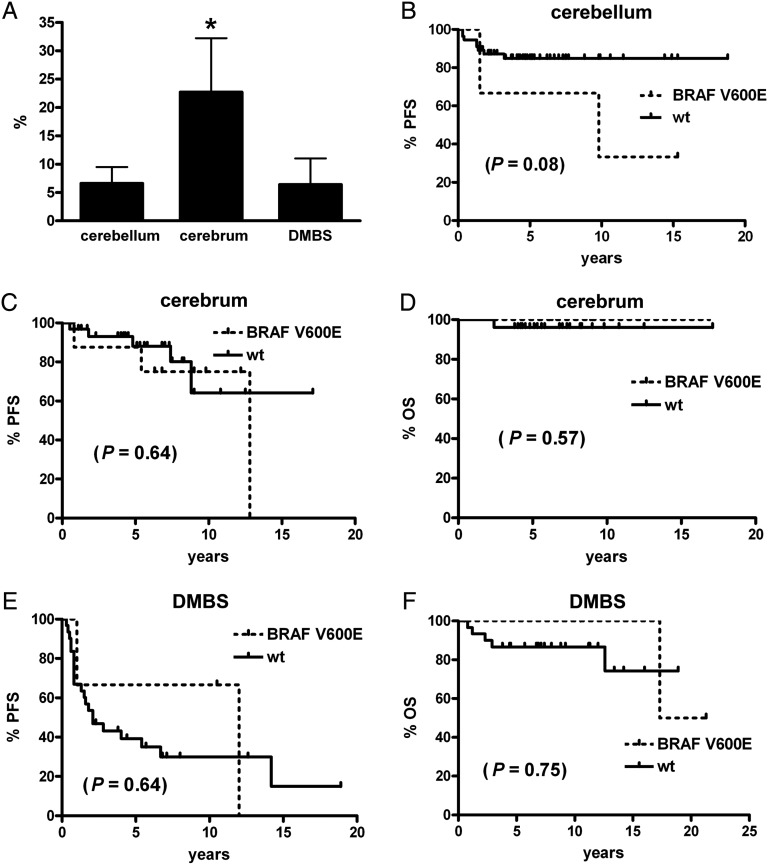
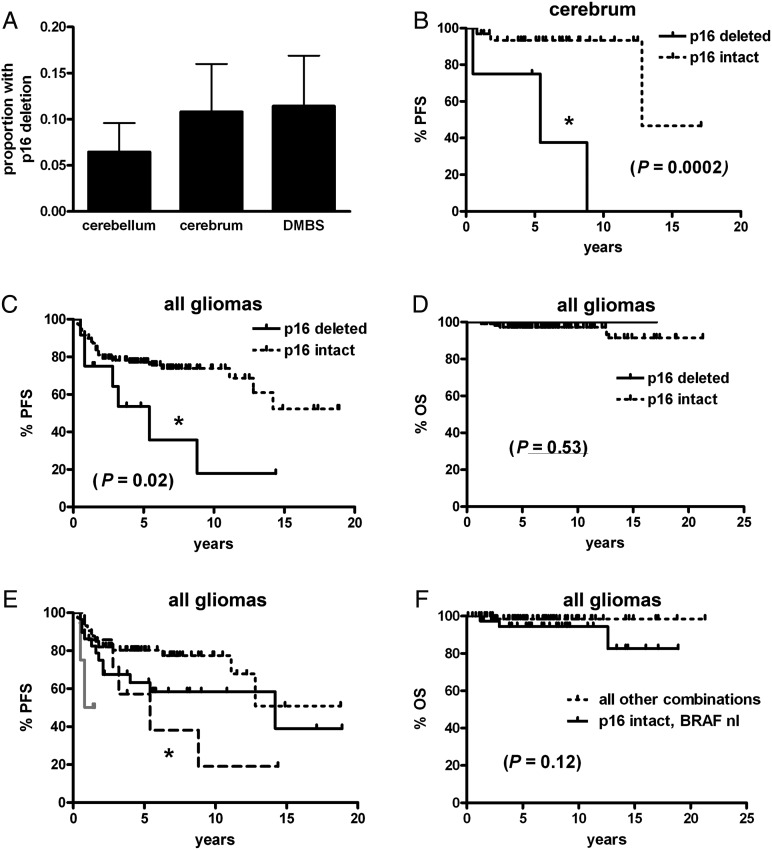
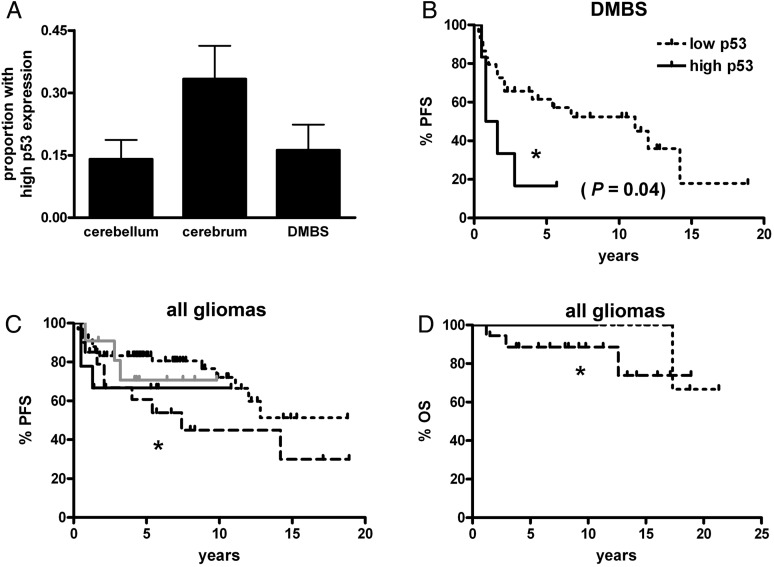
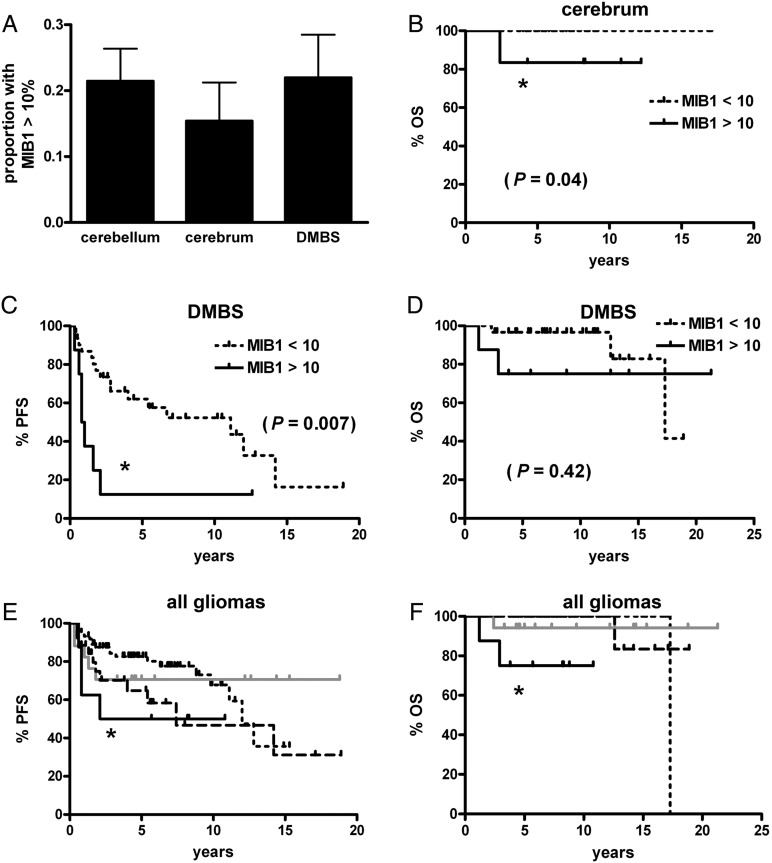
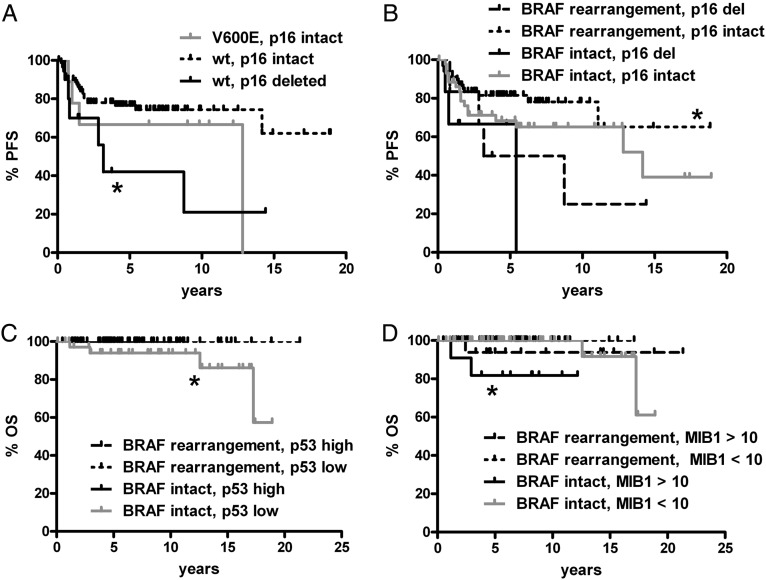
BRAF rearrangements and BRAF V600E point mutations are recurring events in pediatric low-grade gliomas. However, their clinical significance, including possible interactions between these markers and other glioma biomarkers, is unclear. In this study a retrospective cohort of 198 pediatric low-grade gliomas (including 40 treated with adjuvant therapy) was analyzed for BRAF rearrangements, BRAF V600E, p16/CDKN2A deletion, p53 expression, and MIB1 proliferation index. In tumors with BRAF rearrangement, homozygous p16 deletion correlated with shorter progression-free survival (P = .04). A high MIB1 proliferation index trended toward worse response to adjuvant radiotherapy compared to BRAF-rearranged, p16-intact tumors (P = .08). On multivariate analysis, the 2 most consistently powerful independent adverse prognostic markers were midline location (P = .0001) and p16 deletion (P = .03). Tumors with BRAF V600E had a strong trend toward an increased risk for progression (hazard ratio = 2.48, P = .07), whereas those with BRAF rearrangement had a milder trend toward reduced risk (hazard ratio = .54, P = .15). These data suggest that p16 deletion adversely impacts the outcomes of BRAF-driven gliomas, that high proliferation index may be a better marker of progression risk than BRAF, that BRAF rearrangement and BRAF V600E might not necessarily produce comparable outcomes, and that none of these markers is stronger than tumor location in determining prognosis in pediatric low-grade gliomas.
Figures
References
-
- Bar EE, Lin A, Tihan T, Burger PC, Eberhart CG. Frequent gains at chromosome 7q34 involving BRAF in pilocytic astrocytoma. J Neuropathol Exp Neurol. 2008;67:878–887. doi:10.1097/NEN.0b013e3181845622. - DOI - PubMed
-
- Pfister S. BRAF gene duplication constitutes a mechanism of MAPK pathway activation in low-grade astrocytomas. J Clin Invest. 2008;118:1739–1749. doi:10.1172/JCI33656. - DOI - PMC - PubMed
-
- Jones DT, Kocialkowski S, Liu L, et al. Tandem duplication producing a novel oncogenic BRAF fusion gene defines the majority of pilocytic astrocytomas. Cancer Res. 2008;68(21):8673–8677. doi:10.1158/0008-5472.CAN-08-2097. - DOI - PMC - PubMed
-
- Forshew T, Tatevossian RG, Lawson AR, et al. Activation of the ERK/MAPK pathway: a signature genetic defect in posterior fossa pilocytic astrocytomas. J Pathol. 2009;218(2):172–181. doi:10.1002/path.2558. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
