

Long-term dynamics of bone mineral density during intermittent androgen deprivation for men with nonmetastatic, hormone-sensitive prostate cancer
- PMID: 22493411
- PMCID: PMC3383183
- DOI: 10.1200/JCO.2011.38.3745
Long-term dynamics of bone mineral density during intermittent androgen deprivation for men with nonmetastatic, hormone-sensitive prostate cancer
Abstract
Purpose: To investigate changes in bone mineral density (BMD) and fracture risk in men who received intermittent androgen deprivation (IAD) for nonmetastatic, hormone-sensitive prostate cancer.
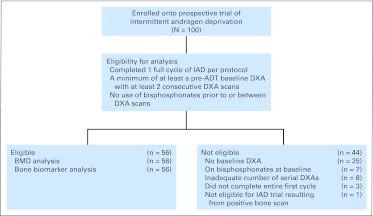
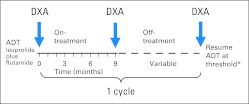
Patients and methods: Men with prostate cancer who lacked radiographically detectable metastases were treated in a prospective trial of IAD. After 9 months of treatment with leuprolide and flutamide, androgen deprivation therapy (ADT) was stopped until prostate-specific antigen reached a threshold (1 ng/mL for radical prostatectomy; 4 ng/mL for radiation or primary ADT) for a new cycle. Dual-energy x-ray absorptiometry (DXA) scans were performed before starting ADT and subsequently with each change in therapy. At least two consecutive DXA scans were required for this analysis. Computed tomography, bone scintigraphy, and lumbar spine x-rays were performed at the beginning and end of each treatment period.
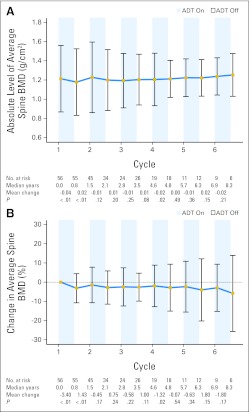
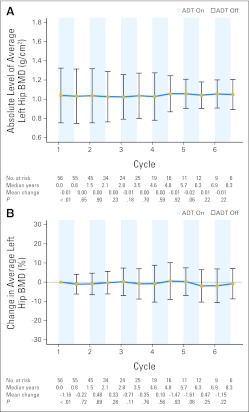
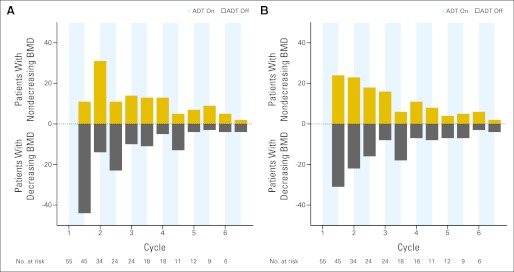
Results: Fifty-six of 100 patients met criteria for this analysis. The median age at study entry was 64.5 years (range, 49.8 to 80.9 years). The average percentage change in BMD during the first on-treatment period was -3.4% (P < .001) for the spine and -1.2% (P = .001) for the left hip. During the first off-treatment period (median, 37.4 weeks; range, 13.4 weeks to 8.7+ years), BMD recovery at the spine was significant, with an average percentage change of +1.4% (P = .002). Subsequent periods had heterogeneous changes of BMD without significant average changes. After a median of 5.5 years (range, 1.1 to 13.8+) years on trial, one patient (1.8%) had a compression fracture associated with trauma.
Conclusion: Patients experienced the greatest average change in BMD during early treatment periods of IAD with a smaller average change thereafter. Fractures were rare.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Heidenreich A, Aus G, Bolla M, et al. EAU guidelines on prostate cancer. Eur Urol. 2008;53:68–80. - PubMed
-
- Loblaw DA, Virgo KS, Nam R, et al. Initial hormonal management of androgen-sensitive metastatic, recurrent, or progressive prostate cancer: 2006 update of an American Society of Clinical Oncology practice guideline. J Clin Oncol. 2007;25:1596–1605. - PubMed
-
- Messing EM, Manola J, Yao J, et al. Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol. 2006;7:472–479. - PubMed
-
- Shahinian VB, Kuo YF, Freeman JL, et al. Increasing use of gonadotropin-releasing hormone agonists for the treatment of localized prostate carcinoma. Cancer. 2005;103:1615–1624. - PubMed
-
- Bolla M. Adjuvant hormonal treatment with radiotherapy for locally advanced prostate cancer. Eur Urol. 1999;35(suppl 1):23–25. discussion 26. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
