

Neoadjuvant treatment response as an early response indicator for patients with rectal cancer
- PMID: 22493423
- PMCID: PMC3383178
- DOI: 10.1200/JCO.2011.39.7901
Neoadjuvant treatment response as an early response indicator for patients with rectal cancer
Abstract
Purpose: Neoadjuvant chemoradiotherapy for rectal cancer is associated with improved local control and may result in complete tumor response. Associations between tumor response and disease control following radical resection should be established before tumor response is used to evaluate treatment strategies. The purpose of this study was to assess and compare oncologic outcomes associated with the degree of pathologic response after chemoradiotherapy.
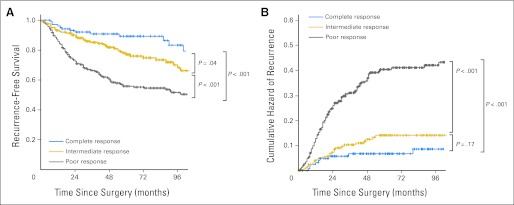
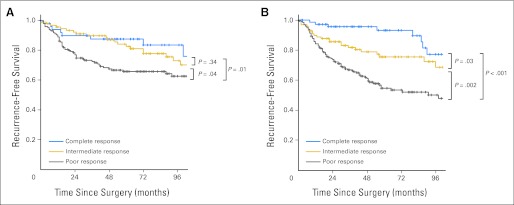
Patients and methods: All patients with locally advanced (cT3-4 or cN+ by endorectal ultrasonography, computed tomography, or magnetic resonance imaging) rectal carcinoma diagnosed from 1993 to 2008 at our institution and treated with preoperative chemoradiotherapy and radical resection were identified, and their records were retrospectively reviewed. The median radiation dose was 50.4 Gy with concurrent chemotherapy. Recurrence-free survival (RFS), distant metastasis (DM), and local recurrence (LR) rates were compared among patients with complete (ypT0N0), intermediate (ypT1-2N0), or poor (ypT3-4 or N+) response by using Kaplan-Meier survival analysis and multivariate Cox proportional hazards regression.
Results: In all, 725 patients were classified by tumor response: complete (131; 18.1%), intermediate (210; 29.0%), and poor (384; 53.0%). Age, sex, cN stage, and tumor location were not related to tumor response. Tumor response (complete v intermediate v poor) was associated with 5-year RFS (90.5% v 78.7% v 58.5%; P < .001), 5-year DM rates (7.0% v 10.1% v 26.5%; P < .001), and 5-year LR only rates (0% v 1.4% v 4.4%; P = .002).
Conclusion: Treatment response to neoadjuvant chemoradiotherapy among patients with locally advanced rectal cancer undergoing radical resection is an early surrogate marker and correlate to oncologic outcomes. These data provide guidance with response-stratified oncologic benchmarks for comparisons of novel treatment strategies.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- American Cancer Society. Atlanta, GA: American Cancer Society; 2011. Cancer Facts & Figures 2011.
-
- National Cancer Institute. Surveillance, Epidemiology, and End Results (SEER) Program ( www.seer.cancer.gov) SEER*Stat Database: Incidence - SEER 17 Regs Public-Use, Nov 2005 Sub (1973-2003 varying). National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2006, based on the November 2005 submission.
-
- O'Connell JB, Maggard MA, Liu JH, et al. Are survival rates different for young and older patients with rectal cancer? Dis Colon Rectum. 2004;47:2064–2069. - PubMed
-
- Das P, Skibber JM, Rodriguez-Bigas MA, et al. Predictors of tumor response and downstaging in patients who receive preoperative chemoradiation for rectal cancer. Cancer. 2007;109:1750–1755. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
