

Low-Dose Treatment with Erythropoiesis-Stimulating Agents and Cardiovascular Geometry in Chronic Kidney Disease: Is Darbepoetin-α More Effective than Expected?
- PMID: 22493599
- PMCID: PMC3318933
- DOI: 10.1159/000334942
Low-Dose Treatment with Erythropoiesis-Stimulating Agents and Cardiovascular Geometry in Chronic Kidney Disease: Is Darbepoetin-α More Effective than Expected?
Abstract
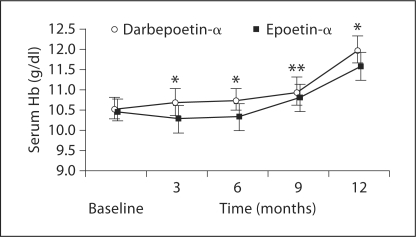
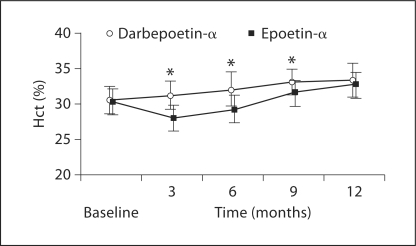
INTRODUCTION: Chronic kidney disease (CKD) is a widespread invalidating condition, leading to erythropoietin deficiency and decreased cardiovascular performance. Darbepoetin-α and epoetin-α are extensively used to correct renal anemia. The aim of this study was to evaluate cardiological outcomes in two groups of CKD patients treated with erythropoiesis-stimulating agents (ESA: 20 μg darbepoetin-α weekly vs. 2,000 IU epoetin-α thrice weekly) with an unconventional 1:300 conversion ratio. METHODS: The study was designed as a single center, retrospective, observational study. One hundred stage IV CKD patients were selected. Hemoglobin (Hb), hematocrit, C-reactive protein, pro-brain natriuretic peptide (BNP) and basal echocardiograms were monitored every 3 months. RESULTS: Darbepoetin-α was significantly more effective in increasing Hb levels after 3 (p < 0.0001), 6 (p < 0.0001), 9 (p < 0.01) and 12 months (p < 0.01) compared to epoetin-α. The optimal Hb target level (11 g/dl < Hb < 12 g/dl) was completely reached after 1 year of treatment with darbepoetin-α and in 70% of the patients treated with epoetin-α (p < 0.01). Cardiovascular performance (left ventricular end-diastolic volume, ejection fraction and pro-BNP) was significantly improved after darbepoetin-α treatment at the 6- and 12-month follow-ups compared to epoetin-α. Discussion: Despite the limitations of a retrospective observational study, these results encourage nephrologists to test the 1:300 darbepoetin/epoetin conversion ratio in 'easy' patients, and aggressive protocols for the treatment of anemia in CKD patients are avoided. Darbepoetin-α appeared effective in anemia correction, improving cardiovascular performance in a significantly higher proportion than epoetin. At low doses, on the other hand, it has to be borne in mind that a treatment regimen with only one submaximal administration per week may increase patient compliance and adherence to therapy, explaining in part the observed results.
Figures
References
-
- National Kidney Foundation K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification and stratification. Am J Kidney Dis. 2002;39(suppl 1):S1–S266. - PubMed
-
- Astor BC, Muntner P, Levin A, Eustace JA, Coresh J. Association of kidney function with anemia: the Third National Health and Nutrition Examination Survey (1988–1994) Arch Intern Med. 2002;162:1401–1408. - PubMed
-
- Nurko S. Anemia in chronic kidney disease: causes, diagnosis, treatment. Clev Clin J Med. 2006;73:289–297. - PubMed
-
- National Kidney Foundation: IV. NKF-K/DOQI Clinical Practice Guidelines for Anemia of Chronic Kidney Disease: update 2008. - PubMed
-
- Levin A, Thompson CR, Ethier J, Carlisle EJ, Tobe S, Mendelssohn D, Burgess E, Jindal K, Barrett B, Singer J, Djurdjev O. Left ventricular mass index increase in early renal disease: impact of decline in hemoglobin. Am J Kidney Dis. 1999;34:125–134. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials