

The effect of enalapril and carvedilol on left ventricular dysfunction in middle childhood and adolescent patients with muscular dystrophy
- PMID: 22493613
- PMCID: PMC3318090
- DOI: 10.4070/kcj.2012.42.3.184
The effect of enalapril and carvedilol on left ventricular dysfunction in middle childhood and adolescent patients with muscular dystrophy
Abstract
Background and objectives: In Duchenne and Becker muscular dystrophies, cardiac function deteriorates with time resulting in heart failure which is often fatal. We prospectively evaluated the effect of enalapril and carvedilol on left ventricular (LV) dysfunction in middle childhood and adolescent patients with muscular dystrophy.
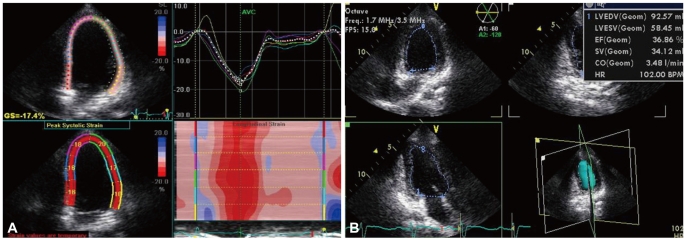
Subjects and methods: Twenty-three patients with LV dysfunction (22 with Duchenne muscular dystrophy, 1 with Becker muscular dystrophy) were enrolled. We prescribed enalapril (13 patients) or carvedilol (10 patients) randomly from July 2008 to August 2010 and followed up the patients until September 2011. The changes in LV function parameters before and after the treatment were evaluated by echocardiography.
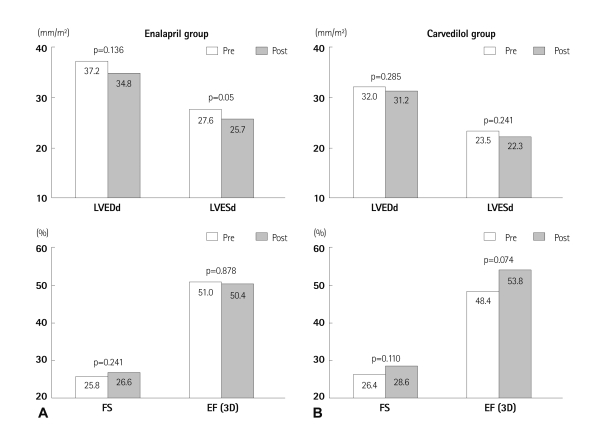
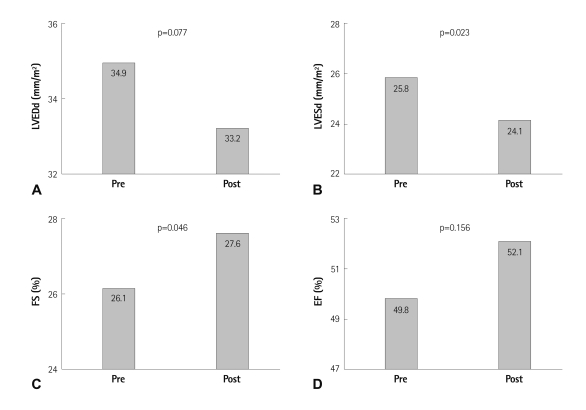
Results: The mean age at the start of treatment with enalapril or carvedilol was 12.6±3.7 years (median 13 years), and mean follow-up duration was 20.1±8.9 months. In the enalapril group, LV fractional shortening (FS) increased from 25.8±2.1 to 26.6±3.0 (p=0.241). In the carvedilol group, LV FS increased from 26.4±1.1 to 28.6±4.2 (p=0.110). In all 23 patients, LV FS significantly increased from 26.1±1.7 (before) to 27.6±3.7 (after treatment) (p<0.046). Indexed LV dimension at end diastole and LV end-diastolic volume decreased slightly, but without statistical significance by tri-plane volumetry. LV diastolic functional parameters were maintained during follow-up period.
Conclusion: Enalapril or carvedilol could improve LV systolic function in middle childhood and adolescent patients with muscular dystrophy without significant adverse effects.
Keywords: Cardiomyopathies; Carvedilol; Echocardiography; Enalapril; Muscular dystrophies.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Emery AE. The muscular dystrophies. Lancet. 2002;359:687–695. - PubMed
-
- Emery AE. Population frequencies of inherited neuromuscular diseases: a world survey. Neuromuscul Disord. 1991;1:19–29. - PubMed
-
- Finsterer J, Stöllberger C. The heart in human dystrophinopathies. Cardiology. 2003;99:1–19. - PubMed
-
- McNally EM. Duchenne muscular dystrophy: how bad is the heart? Heart. 2008;94:976–977. - PubMed
LinkOut - more resources
Full Text Sources
