

Finding the "PR-fect" solution: what is the best tool to measure fetal cardiac PR intervals for the detection and possible treatment of early conduction disease?
- PMID: 22494551
- PMCID: PMC3396786
- DOI: 10.1111/j.1747-0803.2012.00652.x
Finding the "PR-fect" solution: what is the best tool to measure fetal cardiac PR intervals for the detection and possible treatment of early conduction disease?
Abstract
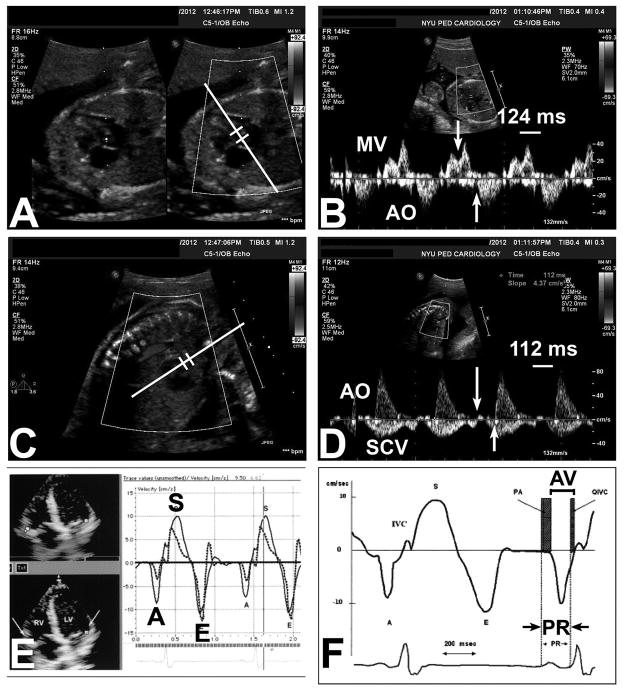
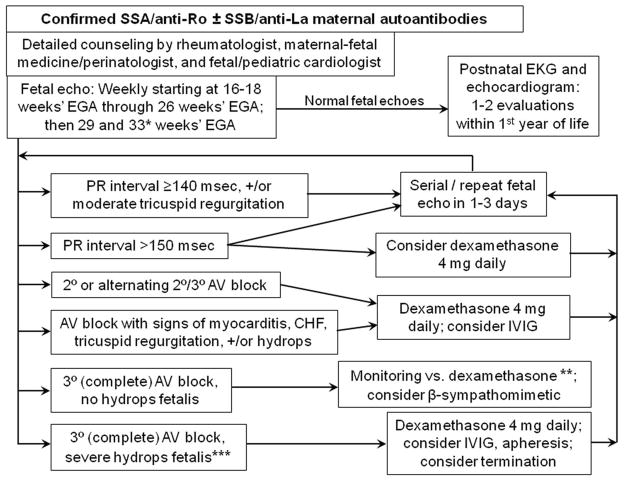
In the absence of structural heart disease, the great majority of cases with complete congenital heart block will be associated with the maternal autoantibodies directed to components of the SSA/Ro-SSB/La ribonucleoprotein complex. Usually presenting in fetal life before 26 weeks' gestation, once third-degree (complete) heart block develops, it is irreversible. Therefore, investigators over the past several years have attempted to predict which fetuses will be at risk for advanced conduction abnormalities by identifying a biomarker for less severe or incomplete disease, in this case, PR interval prolongation or first-degree atrioventricular block. In this state-of-the-art review, we critically analyze the various approaches to defining PR interval prolongation in the fetus, and then analyze several clinical trials that have attempted to address the question of whether complete heart block can be predicted and/or prevented. We find that, first and foremost, definitions of first-degree atrioventricular block vary but that the techniques themselves are all similarly valid and reliable. Nevertheless, the task of predicting those fetuses at risk, and who are therefore candidates for treatment, remains challenging. Of concern, despite anecdotal evidence, there is currently no conclusive proof that a prolonged PR interval predicts complete heart block.
© 2012 Wiley Periodicals, Inc.
Conflict of interest statement
Conflict of Interest: None declared.
Dr. Friedman is on the Speakers Bureau of and is a consultant for, MedImmune.
Figures
References
-
- Jaeggi ET, Silverman ED, Yoo S-J, Kingdom J. Is immune-mediated complete fetal atrioventricular block reversible by transplacental dexamethasone therapy? Ultrasound Obstet Gynecol. 2004;23:602–605. - PubMed
-
- Gordon PA. Congenital heart block: clinical features and therapeutic approaches. Lupus. 2007;16:642–646. - PubMed
-
- Bruer JMPJ, Kapusta L, Stoutenbeek P, Visser GHA, Van den Berg P, Meijboom EJ. Isolated congenital complete atrioventricular block diagnosed in utero: Natural history and outcome. J Mat Fetal Neonat Med. 2008;21:469–476. - PubMed
-
- Mevorach D, Elchalal U, Rein AJJT. Prevention of complete heart block in children of mothers with anti-SSA/Ro and anti-SSB/La autoantibodies: detection and treatment of first-degree atrioventricular block. Curr Opin Rheumatol. 2009;21:478–482. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
