

Drug repositioning for personalized medicine
- PMID: 22494857
- PMCID: PMC3446277
- DOI: 10.1186/gm326
Drug repositioning for personalized medicine
Abstract
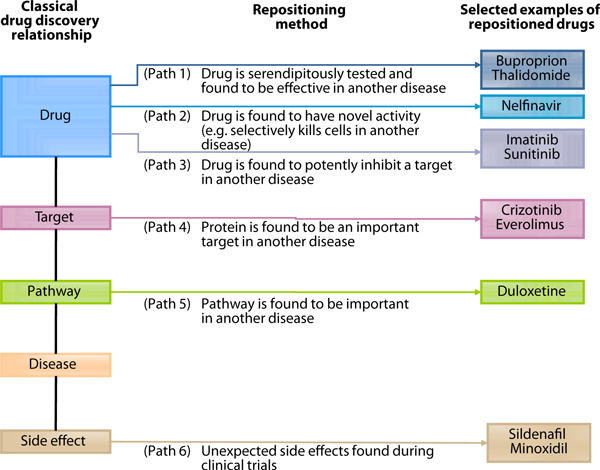
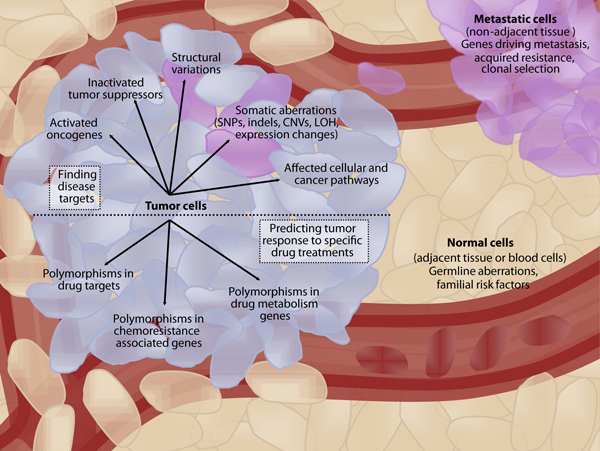
Human diseases can be caused by complex mechanisms involving aberrations in numerous proteins and pathways. With recent advances in genomics, elucidating the molecular basis of disease on a personalized level has become an attainable goal. In many cases, relevant molecular targets will be identified for which approved drugs already exist, and the potential repositioning of these drugs to a new indication can be investigated. Repositioning is an accelerated route for drug discovery because existing drugs have established clinical and pharmacokinetic data. Personalized medicine and repositioning both aim to improve the productivity of current drug discovery pipelines, which expend enormous time and cost to develop new drugs, only to have them fail in clinical trials because of lack of efficacy or toxicity. Here, we discuss the current state of research in these two fields, focusing on recent large-scale efforts to systematically find repositioning candidates and elucidate individual disease mechanisms in cancer. We also discuss scenarios in which personalized drug repositioning could be particularly rewarding, such as for diseases that are rare or have specific mutations, as well as current challenges in this field. With an increasing number of drugs being approved for rare cancer subtypes, personalized medicine and repositioning approaches are poised to significantly alter the way we diagnose diseases, infer treatments and develop new drugs.
Keywords: Personalized medicine; cancer; computational drug design; drug discovery; high-throughput screening; orphan diseases; repositioning; repurposing.
Figures
References
-
- Lawrence S. Drug output slows in 2006. Nat Biotechnol. 2007;25:1073. doi: 10.1038/nbt1007-1073. - DOI
-
- Paul SM, Mytelka DS, Dunwiddie CT, Persinger CC, Munos BH, Lindborg SR, Schacht AL. How to improve R&D productivity: the pharmaceutical industry's grand challenge. Nat Rev Drug Discov. 2010;9:203–214. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
