

Fatal and near-fatal asthma in children: the critical care perspective
- PMID: 22494876
- PMCID: PMC3402707
- DOI: 10.1016/j.jpeds.2012.02.041
Fatal and near-fatal asthma in children: the critical care perspective
Abstract
Objective: To characterize the clinical course, therapies, and outcomes of children with fatal and near-fatal asthma admitted to pediatric intensive care units (PICUs).
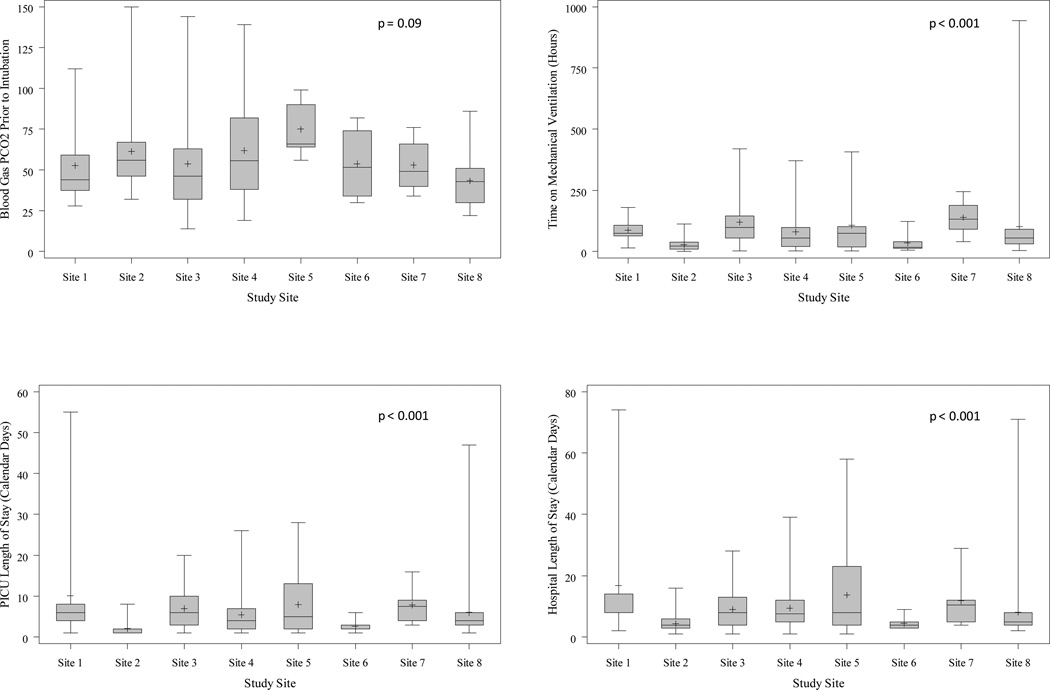
Study design: This was a retrospective chart abstraction across the 8 tertiary care PICUs of the Collaborative Pediatric Critical Care Research Network (CPCCRN). Inclusion criteria were children (aged 1-18 years) admitted between 2005 and 2009 (inclusive) for asthma who received ventilation (near-fatal) or died (fatal). Data collected included medications, ventilator strategies, concomitant therapies, demographic information, and risk variables.
Results: Of the 261 eligible children, 33 (13%) had no previous history of asthma, 218 (84%) survived with no known complications, and 32 (12%) had complications. Eleven (4%) died, 10 of whom had experienced cardiac arrest before admission. Patients intubated outside the PICU had a shorter duration of ventilation (median, 25 hours vs 84 hours; P < .001). African-Americans were disproportionately represented among the intubated children and had a shorter duration of intubation. Barotrauma occurred in 15 children (6%) before admission. Pharmacologic therapy was highly variable, with similar outcomes.
Conclusion: Of the children ventilated in the CPCCRN PICUs, 96% survived to hospital discharge. Most of the children who died experienced cardiac arrest before admission. Intubation outside the PICU was correlated with shorter duration of ventilation. Complications of barotrauma and neuromyopathy were uncommon. Practice patterns varied widely among the CPCCRN sites.
Copyright © 2012 Mosby, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
Near-fatal asthma: an ounce of prevention may be worth more than a pound of cure.J Pediatr. 2012 Aug;161(2):182-4. doi: 10.1016/j.jpeds.2012.04.038. Epub 2012 May 24. J Pediatr. 2012. PMID: 22632877 No abstract available.
References
-
- Bohn D, Kissoon N. Acute asthma. Pediatr Crit Care Med. 2001;2:151–163. - PubMed
-
- EPR-3.Expert panel report 3, National Institutes of Health, National Heart Lung and Blood Institute, National Asthma Education and Prevention Program. Guidelines for the diagnosis and management of asthma (EPR-3 2007). NIH Publication No. 08-4051. Bethesda, MD: [Accessed January 8, 2012]. http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm.
-
- Roberts JS, Bratton SL, Brogan TV. Acute severe asthma: differences in therapies and outcomes among pediatric intensive care units. Crit Care Med. 2002;30:581–585. - PubMed
-
- Bratton SL, Odetola FO, McCollegan J, Cabana MD, Levy FH, Keenan HT. Regional variation in ICU care for pediatric patients with asthma. J Pediatr. 2005;147:355–361. - PubMed
-
- Bratton SL, Roberts JS. Variation in the use of mechanical ventilation for asthma: how big a gap? Pediatr Crit Care Med. 2007;8:186–187. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD050012/HD/NICHD NIH HHS/United States
- U10-HD050096/HD/NICHD NIH HHS/United States
- U10 HD049981/HD/NICHD NIH HHS/United States
- U10 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
- U10-HD063106/HD/NICHD NIH HHS/United States
- U10 HD063106/HD/NICHD NIH HHS/United States
- UG1 HD063108/HD/NICHD NIH HHS/United States
- RL1 HD107773/HD/NICHD NIH HHS/United States
- U10-HD050012/HD/NICHD NIH HHS/United States
- U10-HD063114/HD/NICHD NIH HHS/United States
- U10 HD063114/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- U10 HD063108/HD/NICHD NIH HHS/United States
- U10-HD063108/HD/NICHD NIH HHS/United States
- U10-HD049983/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- UG1 HD049981/HD/NICHD NIH HHS/United States
- U10-HD049981/HD/NICHD NIH HHS/United States
