

Sympathetic inhibition attenuates hypoxia induced insulin resistance in healthy adult humans
- PMID: 22495590
- PMCID: PMC3424732
- DOI: 10.1113/jphysiol.2011.227090
Sympathetic inhibition attenuates hypoxia induced insulin resistance in healthy adult humans
Abstract
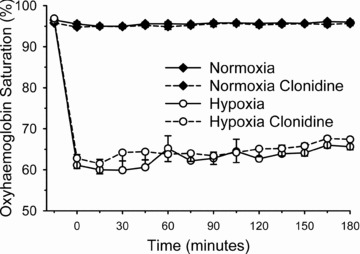
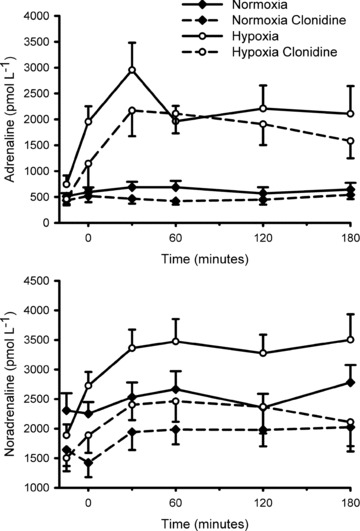
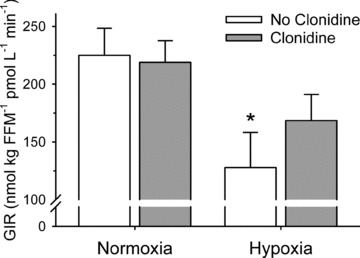
Acute exposure to hypoxia decreases insulin sensitivity in healthy adult humans; the mechanism is unclear, but increased activation of the sympathetic nervous system may be involved. We have investigated the hypothesis that short-term sympathetic inhibition attenuates hypoxia induced insulin resistance. Insulin sensitivity (via the hyperinsulinaemic euglycaemic clamp) was determined in 10 healthy men (age 23 ± 1 years, body mass index 24.2 ± 0.8 kg m⁻² (means ± SEM)), in a random order, during normoxia (FIO₂ =0.21), hypoxia (FIO₂ =0.11), normoxia and sympathetic inhibition (via 48 h transdermal administration of the centrally acting α2-adrenergic receptor agonist, clonidine), and hypoxia and sympathetic inhibition.Oxyhaemoglobin saturation (pulse oximetry) was decreased (P<0.001) with hypoxia (63 ± 2%) compared with normoxia (96 ± 0%), and was unaffected by sympathetic inhibition (P>0.25). The area under the noradrenaline curve (relative to the normoxia response) was increased with hypoxia (137 ± 13%; P =0.02); clonidine prevented the hypoxia induced increase (94 ± 14%; P =0.43). The glucose infusion rate (adjusted for fat free mass and circulating insulin concentration) required to maintain blood glucose concentration at 5 mmol l⁻¹ during administration of insulin was decreased in hypoxia compared with normoxia (225 ± 23 vs. 128 ± 30 nmol (kg fat free mass)⁻¹ pmol l⁻¹ min⁻¹; P =0.03), and unchanged during normoxia and sympathetic inhibition (219 ± 19; P =0.86) and hypoxia and sympathetic inhibition (169 ± 23; P =0.23). We conclude that short-term sympathetic inhibition attenuates hypoxia induced insulin resistance.
Figures
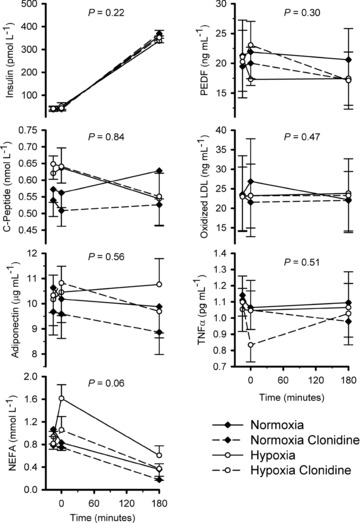
 and clonidine. NEFA: non-esterified fatty acids. PEDF: pigment epithelium derived factor. LDL: low density lipoprotein. TNFα: tumour necrosis factor α.
and clonidine. NEFA: non-esterified fatty acids. PEDF: pigment epithelium derived factor. LDL: low density lipoprotein. TNFα: tumour necrosis factor α.References
-
- Bell C. Pigment epithelium-derived factor: a not so sympathetic regulator of insulin resistance? Exerc Sport Sci Rev. 2011;39:187–190. - PubMed
-
- Bloomgarden ZT. Measures of insulin sensitivity. Clin Lab Med. 2006;26:611–633. - PubMed
-
- Braun B, Rock PB, Zamudio S, Wolfel GE, Mazzeo RS, Muza SR, Fulco CS, Moore LG, Butterfield GE. Women at altitude: short-term exposure to hypoxia and/or α1-adrenergic blockade reduces insulin sensitivity. J Appl Physiol. 2001;91:623–631. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous