

doi: 10.1259/bjr/21382039.
Epub 2012 Apr 11.
Perforated tumours in the gastrointestinal tract: CT findings and clinical implications
Affiliations
- PMID: 22496070
- PMCID: PMC3487063
- DOI: 10.1259/bjr/21382039
Item in Clipboard
Perforated tumours in the gastrointestinal tract: CT findings and clinical implications
Br J Radiol.
2012 Sep.
Abstract
Perforation usually requires emergency surgery and may affect the prognosis of patients with gastrointestinal tumours. Accurate pre-operative diagnosis of these conditions is important because proper management such as curative surgical treatment may be needed. The aims of this article are to illustrate CT appearances of perforated tumours of the gastrointestinal tract and to discuss their impact on clinical management.
Figures
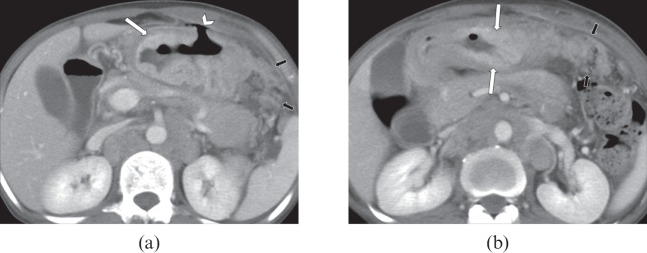
A 55-year-old female with a perforated gastric adenocarcinoma. (a, b) Axial CT scans show a focal wall defect at the anterior wall of the gastric antrum with a small amount of air around the perforation site (arrowhead). Enhanced wall thickening of the gastric antrum is seen (large arrows). Note infiltrating lesions of soft-tissue attenuation in the adjacent omentum, indicating peritoneal dissemination (small arrows).
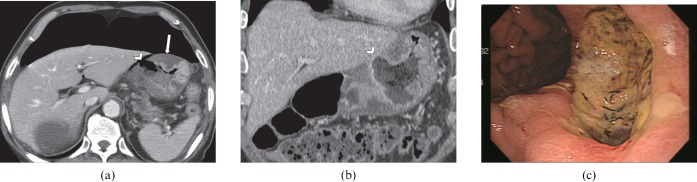
A 75-year-old male with a perforated gastric adenocarcinoma. (a) Axial CT scan shows a large quantity of extraluminal air anterior to the liver and stomach and a focal wall defect at the gastric body (arrowhead). Findings of oedematous wall thickening of the stomach (arrow) with scant perigastric fat infiltration observed in this case are not distinguishable from those of benign gastric perforation. (b) After primary closure of the gastric perforation, a large, deep ulceration is seen at the gastric body on the coronal CT image (arrowhead). (c) Gastroscopy revealed a large, deep ulceration at the body portion. Poorly differentiated adenocarcinoma without evidence of peritoneal metastasis was confirmed by pathology.
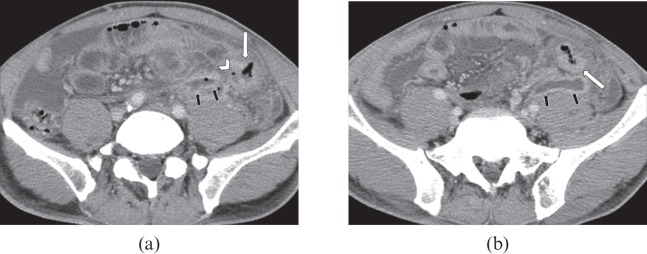
A 52-year-old male with a perforated adenocarcinoma in the sigmoid colon. (a, b) Axial CT scans show irregular enhanced wall thickening of the sigmoid colon (large arrows) and a focal wall defect at the medial aspect (arrowhead). A small abscess is seen above the left psoas muscle (small arrows).
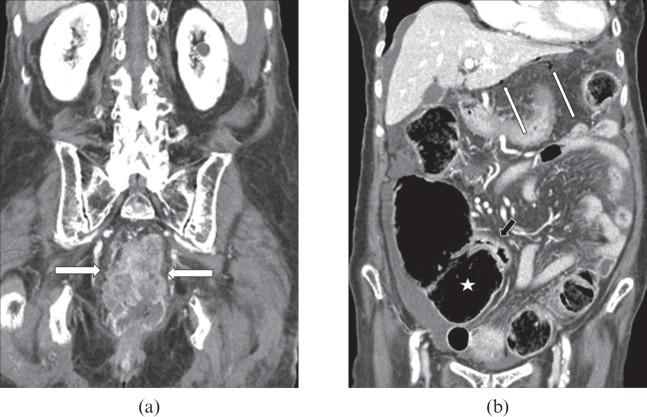
A 99-year-old female with a colonic closed-loop obstruction secondary to rectal adenocarcinoma. (a) Coronal CT image shows an irregular enhancing mass in the rectum (arrows). (b) Marked luminal distension of the caecum (asterisk) and proximal ascending colon, and collapsed lumen of the terminal ileum (small arrow) are observed on a coronal CT image. Note free air bubbles (long arrows) in the left subhepatic space and ascites. Subsequently, an emergency operation revealed multiple perforations in the caecum.
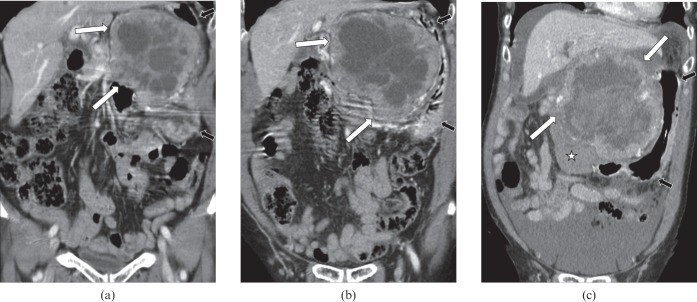
A 79-year-old female with a ruptured gastrointestinal stromal tumour (GIST). (a) Coronal CT image demonstrates a large heterogeneous mass (large arrows) which shows an exophytic growth from the stomach (small arrows). Multifocal low-attenuation areas, corresponding to necrosis, with septa are seen within the tumour. The patient refused surgery. (b) Coronal CT image obtained 10 months later shows the interval growth of the mass (large arrows) abutting the stomach (small arrows). (c) A further 10 months later, the patient attended the emergency department of our hospital owing to development of acute abdominal pain. Internal high-attenuation haemorrhage was newly seen in the mass (large arrows) abutting the stomach (small arrows) on a coronal image. A large amount of high-attenuation ascites representing haemoperitoneum and clotted blood adjacent to the mass (asterisk) was also seen. A ruptured, high-risk GIST with haemorrhagic necrosis was confirmed pathologically after surgical resection of the tumour.
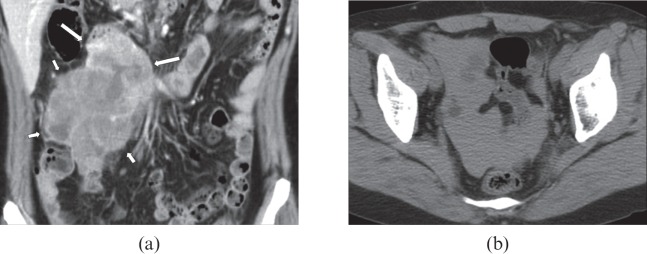
A 48-year-old female with a ruptured gastrointestinal stromal tumour (GIST). (a) Coronal reformatted enhanced CT image shows a large, irregular contoured mass with heterogeneous enhancement abutting the ileum. Note the slightly decreased enhancement in the lower lateral aspect of the mass (small arrows) compared with that of the upper medial portion (large arrows). (b) Pre-contrast scan shows high-attenuation fluid representing haemoperitoneum in the pelvic cavity. On pathological examination, this mass showed necrosis and rupture, corresponding to the lower portion of the mass. This mass was confirmed as a high-risk GIST.
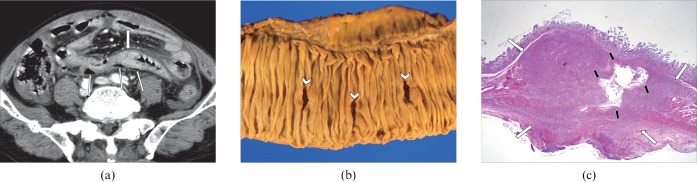
A 79-year-old male with primary lung cancer (squamous cell carcinoma) presenting with acute abdominal pain. (a) Axial CT scan shows suspected focal wall thickening in the jejunum (wide arrow). Extraluminal air bubbles are seen around this jejunal loop (thin arrows). (b) The resected specimen shows three perforation sites induced by mucosal ulcerations (arrowheads). (c) Low-power photomicrograph (haematoxylin and eosin stain, ×4) shows metastatic tumour infiltration mainly in the subepithelial layers, resulting in a bulging contour (large arrows). An irregular necrotic portion, connected to a mucosal ulceration, was found within the tumour (small arrows).
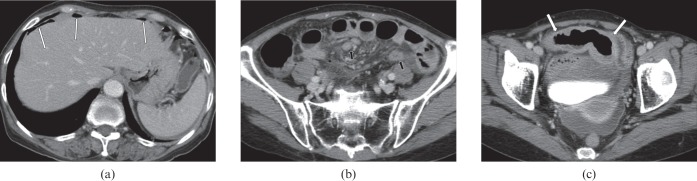
A 71-year-old female with a perforated peripheral T-cell lymphoma in the ileum. (a–c) Axial CT images demonstrate segmental, isoattenuated wall thickening of the ileum, which shows a mildly dilated lumen (arrows on c). Also note free air around the liver (thin arrows on a), enlarged mesenteric lymph nodes (small arrows on b) and mesenteric haziness (b). Perforation was found at surgery.
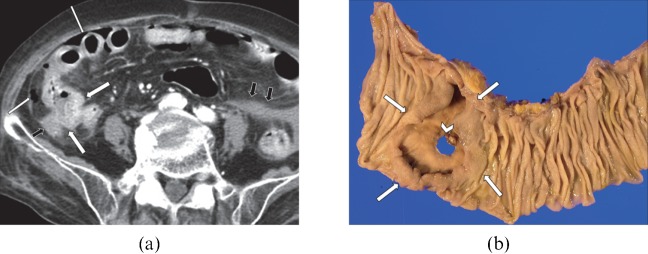
An 83-year-old female with perforated diffuse large B-cell lymphoma in the ileum. (a) Axial CT image shows mild wall thickening of the ileum in the right lower quadrant area (arrows). Multifocal free air (long arrows) and ascites (short arrows) are found in the peritoneal cavity. (b) The specimen shows a mass (arrows) with central perforation (arrowhead) in the ileum. This mass was confirmed pathologically as diffuse large B-cell lymphoma.
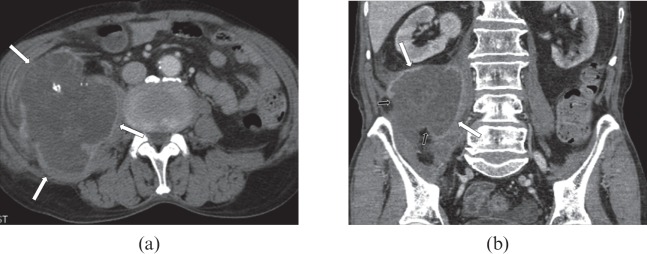
An 82-year-old male with a perforated mucinous adenocarcinoma of the appendix. (a) Axial and (b) coronal CT images show a large, low-attenuation mass with intratumoral calcifications (arrows) in the right lower quadrant. This mass extends to the right psoas muscle. Note the retroperitoneal spread of mucin through the discontinuity of the thin enhanced wall in the mass (small arrows on b).
Similar articles
-
CT diagnosis of non-traumatic gastrointestinal perforation: an emphasis on the causes.Jpn J Radiol. 2020 Feb;38(2):101-111. doi: 10.1007/s11604-019-00910-7. Epub 2019 Dec 17. Jpn J Radiol. 2020. PMID: 31848888 Review.
-
A Perforated Small Bowel GI Stromal Tumor: An Unsuspecting Diagnosis in a Patient with Focal Peritonitis.Am Surg. 2020 Apr 1;86(4):e208-e209. Am Surg. 2020. PMID: 32391782 No abstract available.
-
Delayed Perforation After Endoscopic Resection of Upper Gastrointestinal Tumors: CT Findings to Identify Patients Requiring Surgery.J Clin Gastroenterol. 2025 Jul 1;59(6):542-548. doi: 10.1097/MCG.0000000000002037. J Clin Gastroenterol. 2025. PMID: 38896425
-
Gastrointestinal tract perforation: evaluation of MDCT according to perforation site and elapsed time.Eur Radiol. 2014 Jun;24(6):1386-93. doi: 10.1007/s00330-014-3115-z. Epub 2014 Mar 13. Eur Radiol. 2014. PMID: 24623365
-
Gastrointestinal tract perforation: MDCT findings according to the perforation sites.Korean J Radiol. 2009 Jan-Feb;10(1):63-70. doi: 10.3348/kjr.2009.10.1.63. Korean J Radiol. 2009. PMID: 19182505 Free PMC article. Review.
Cited by
-
Multimodality imaging of adult gastric emergencies: A pictorial review.Indian J Radiol Imaging. 2017 Jan-Mar;27(1):13-22. doi: 10.4103/0971-3026.202957. Indian J Radiol Imaging. 2017. PMID: 28515579 Free PMC article.
-
An unusual case of diastatic perforation of the transverse colon: Case report and literature review.Radiol Case Rep. 2024 Mar 28;19(6):2434-2437. doi: 10.1016/j.radcr.2024.02.109. eCollection 2024 Jun. Radiol Case Rep. 2024. PMID: 38585400 Free PMC article.
-
Free abdominal gas on computed tomography in the emergency department: aetiologies and association between amount of free gas and mortality.Ann R Coll Surg Engl. 2020 Oct;102(8):581-589. doi: 10.1308/rcsann.2020.0057. Epub 2020 Apr 1. Ann R Coll Surg Engl. 2020. PMID: 32233866 Free PMC article.
-
Unsuspected colorectal carcinoma on routine abdominopelvic computed tomography.Singapore Med J. 2015 May;56(5):248-56; quiz 257. doi: 10.11622/smedj.2015072. Singapore Med J. 2015. PMID: 26034316 Free PMC article. Review.
-
CT diagnosis of non-traumatic gastrointestinal perforation: an emphasis on the causes.Jpn J Radiol. 2020 Feb;38(2):101-111. doi: 10.1007/s11604-019-00910-7. Epub 2019 Dec 17. Jpn J Radiol. 2020. PMID: 31848888 Review.
References
-
- Cegarra-Navarro MF, de laCalle MA, Girela-Baena E, García-Santos JM, Lloret-Estañ F, de Andrés EP. Ruptured gastrointestinal stromal tumors: radiologic findings in six cases. Abdom Imaging 2005;30:535–42 - PubMed
-
- Chao TC, Chao HH, Jan YY, Chen MF. Perforation through small bowel malignant tumors. J Gastrointest Surg 2005;9:430–5 - PubMed
-
- Hohenberger P, Ronellenfitsch U, Oladeji O, Pink D, Ströbel P, Wardelmann E, et al. Pattern of recurrence in patients with ruptured primary gastrointestinal stromal tumour. Br J Surg 2010;97:1854–9 - PubMed
-
- Byun JH, Ha HK, Kim AY, Kim TK, Ko EY, Lee JK, et al. CT findings in peripheral T-cell lymphoma involving the gastrointestinal tract. Radiology 2003;227:59–67 - PubMed
