

Magnetic resonance imaging with 3-dimensional analysis of left ventricular remodeling in isolated mitral regurgitation: implications beyond dimensions
- PMID: 22496130
- PMCID: PMC3939018
- DOI: 10.1161/CIRCULATIONAHA.111.073239
Magnetic resonance imaging with 3-dimensional analysis of left ventricular remodeling in isolated mitral regurgitation: implications beyond dimensions
Abstract
Background: Although surgery is indicated in patients with mitral regurgitation (MR) when left ventricular (LV) end-systolic (LVES) dimension is >40 mm, LV ejection fraction may decrease after mitral valve surgery. We hypothesize that significant LV remodeling before surgery is not reflected by standard echocardiographic parameters measured at the base of the heart.
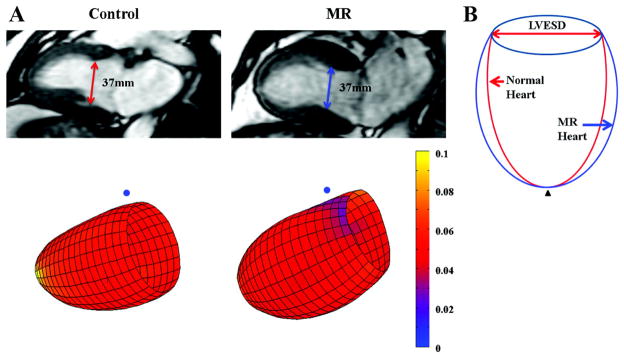
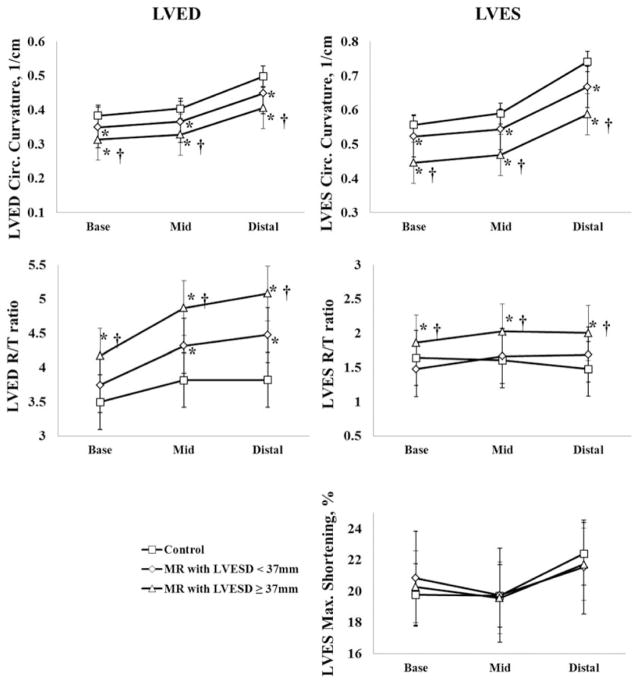
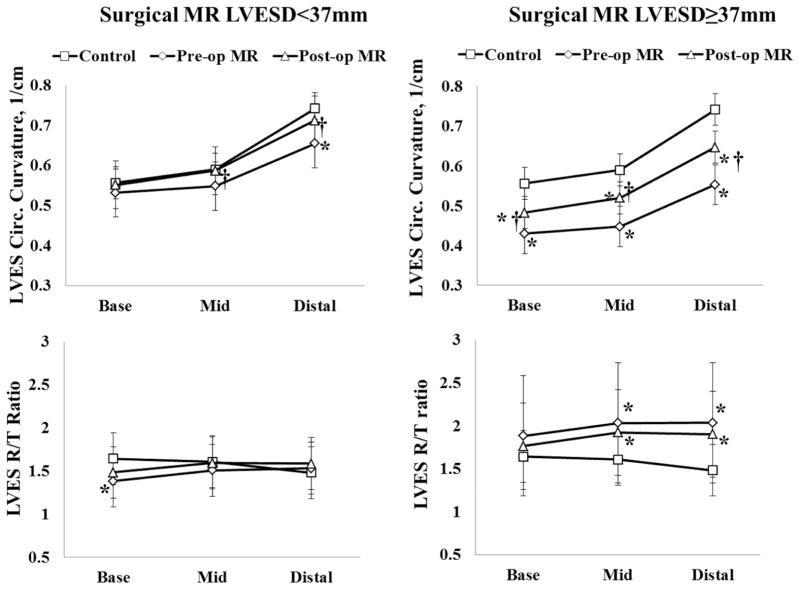
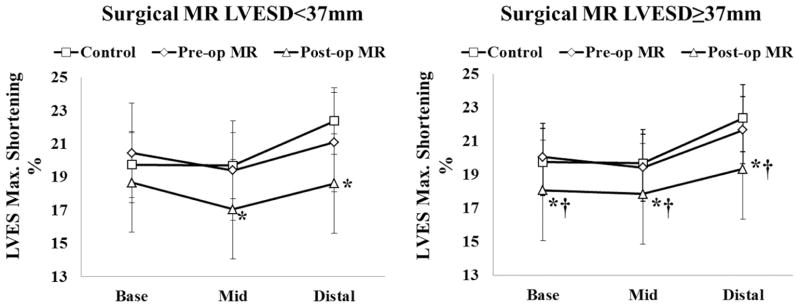
Methods and results: Ninety-four patients (age, 54 ± 11 years; 38% female) with degenerative isolated MR underwent cine magnetic resonance imaging with tissue tagging and 3-dimensional analysis. In 51 control subjects (age, 44 ± 14 years; 53% female), the relation between LVES volume (LVESV) and LVES dimension was quadratic, whereas in 94 MR patients, this relation was cubic, indicating a greater increase in LVESV per LVES dimension among MR patients. Moreover, magnetic resonance imaging LVESV from summated serial short-axis slices was significantly greater than LVESV assessed with the Bullet formula in MR patients, attributed to a more spherical remodeling distal to the tips of the papillary muscles (P<0.001). Thirty-five patients underwent mitral valve repair per current guideline recommendations. LV ejection fraction decreased from 61 ± 7% to 54 ± 8% (P<0.0001) and maximum shortening decreased significantly below normal at 1 year postoperatively (P<0.0001). Despite normalization of LV stroke volume and LV end-diastolic volume/mass ratio, there was a persistent significant increase in distal LVES 3-dimensional radius/wall thickness ratio and LVESV index after surgery.
Conclusions: Despite apparently preserved LVES dimension, MR patients demonstrate significant spherical mid to apical LVES remodeling that contributes to higher LVESV than predicted by standard geometry-based calculations. Decreased LV strain after surgery suggests that a volumetric analysis of LV remodeling and function may be preferred to evaluate disease progression in isolated MR.
Conflict of interest statement
Figures


Comment in
-
Letter by Vallakati and Sharma regarding article, "magnetic resonance imaging with 3-dimensional analysis of left ventricular remodeling in isolated mitral regurgitation: implications beyond dimensions".Circulation. 2013 Feb 19;127(7):e461. doi: 10.1161/CIRCULATIONAHA.112.119800. Circulation. 2013. PMID: 23429901 No abstract available.
-
Response to letter regarding article, “magnetic resonance imaging with 3-dimensional analysis of left ventricular remodeling in isolated mitral regurgitation: implications beyond dimensions”.Circulation. 2013 Feb 19;127(7):e462. doi: 10.1161/circulationaha.112.134858. Circulation. 2013. PMID: 23550297 No abstract available.
Similar articles
-
Increased oxidative stress and cardiomyocyte myofibrillar degeneration in patients with chronic isolated mitral regurgitation and ejection fraction >60%.J Am Coll Cardiol. 2010 Feb 16;55(7):671-9. doi: 10.1016/j.jacc.2009.08.074. J Am Coll Cardiol. 2010. PMID: 20170794 Free PMC article.
-
Assessment of Left Ventricular Reverse Remodeling by Cardiac MRI in Patients Undergoing Repair Surgery for Severe Aortic or Mitral Regurgitation.J Cardiothorac Vasc Anesth. 2019 Jul;33(7):1901-1911. doi: 10.1053/j.jvca.2018.11.013. Epub 2018 Nov 14. J Cardiothorac Vasc Anesth. 2019. PMID: 30583928
-
Left ventricular remodeling after mini-mitral repair-does the complexity of mitral disease matter?J Card Surg. 2019 Oct;34(10):913-918. doi: 10.1111/jocs.14146. Epub 2019 Jul 3. J Card Surg. 2019. PMID: 31269266
-
Disparities in quantification of mitral valve regurgitation between cardiovascular magnetic resonance imaging and trans-thoracic echocardiography: a systematic review.Int J Cardiovasc Imaging. 2025 Apr;41(4):647-658. doi: 10.1007/s10554-024-03280-y. Epub 2024 Nov 5. Int J Cardiovasc Imaging. 2025. PMID: 39499451 Free PMC article.
-
Mechanism of recurrent ischemic mitral regurgitation after annuloplasty: continued LV remodeling as a moving target.Circulation. 2004 Sep 14;110(11 Suppl 1):II85-90. doi: 10.1161/01.CIR.0000138192.65015.45. Circulation. 2004. PMID: 15364844 Review.
Cited by
-
Importance of three-dimensional geometric analysis in the assessment of the athlete's heart.Am J Cardiol. 2013 Apr 1;111(7):1067-72. doi: 10.1016/j.amjcard.2012.12.027. Epub 2013 Jan 17. Am J Cardiol. 2013. PMID: 23332597 Free PMC article.
-
Left Ventricular Ejection Index as a Marker of Early Myocardial Dysfunction in Primary Mitral Regurgitation: Novel or Old in Disguise?Circ Cardiovasc Imaging. 2015 Sep;8(9):e003995. doi: 10.1161/CIRCIMAGING.115.003995. Circ Cardiovasc Imaging. 2015. PMID: 26338880 Free PMC article. No abstract available.
-
A prospective study examining the role of myocardial Fibrosis in outcome following mitral valve repair IN DEgenerative mitral Regurgitation: rationale and design of the mitral FINDER study.BMC Cardiovasc Disord. 2017 Nov 22;17(1):282. doi: 10.1186/s12872-017-0715-y. BMC Cardiovasc Disord. 2017. PMID: 29166877 Free PMC article. Clinical Trial.
-
Left ventricular twist and shear in patients with primary mitral regurgitation.J Magn Reson Imaging. 2015 Aug;42(2):400-6. doi: 10.1002/jmri.24811. Epub 2014 Nov 19. J Magn Reson Imaging. 2015. PMID: 25408263 Free PMC article.
-
Multiscale Finite Element Modeling of Left Ventricular Growth in Simulations of Valve Disease.Ann Biomed Eng. 2024 Aug;52(8):2024-2038. doi: 10.1007/s10439-024-03497-x. Epub 2024 Apr 2. Ann Biomed Eng. 2024. PMID: 38564074 Free PMC article.
References
-
- Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368:1005–1011. - PubMed
-
- Enriquez-Sarano M, Akins CW, Vahanian A. Mitral regurgitation. Lancet. 2009;373:1382–1394. - PubMed
-
- Enriquez-Sarano M, Tajik AJ, Schaff HV, Orszulak TA, McGoon MD, Bailey KR, Frye RL. Echocardiographic prediction of left ventricular function after correction of mitral regurgitation: results and clinical implications. J Am Coll Cardiol. 1994;24:1536–1543. - PubMed
-
- Borer JS, Bonow RO. Contemporary approach to aortic and mitral regurgitation. Circulation. 2003;108:2432–2438. - PubMed
-
- Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O’Gara PT, O’Rourke RA, Otto CM, Shah PM, Shanewise JS, Smith SC, Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48:e1–148. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
