

Does this adult patient have a blunt intra-abdominal injury?
- PMID: 22496266
- PMCID: PMC4966670
- DOI: 10.1001/jama.2012.422
Does this adult patient have a blunt intra-abdominal injury?
Abstract
Context: Blunt abdominal trauma often presents a substantial diagnostic challenge. Well-informed clinical examination can identify patients who require further diagnostic evaluation for intra-abdominal injuries after blunt abdominal trauma.
Objective: To systematically assess the precision and accuracy of symptoms, signs, laboratory tests, and bedside imaging studies to identify intra-abdominal injuries in patients with blunt abdominal trauma.
Data sources: We conducted a structured search of MEDLINE (1950-January 2012) and EMBASE (1980-January 2012) to identify English-language studies examining the identification of intra-abdominal injuries. A separate, structured search was conducted for studies evaluating bedside ultrasonography.
Study selection: We included studies of diagnostic accuracy for intra-abdominal injury that compared at least 1 finding with a reference standard of abdominal computed tomography, diagnostic peritoneal lavage, laparotomy, autopsy, and/or clinical course for intra-abdominal injury. Twelve studies on clinical findings and 22 studies on bedside ultrasonography met inclusion criteria for data extraction.
Data extraction: Critical appraisal and data extraction were independently performed by 2 authors.
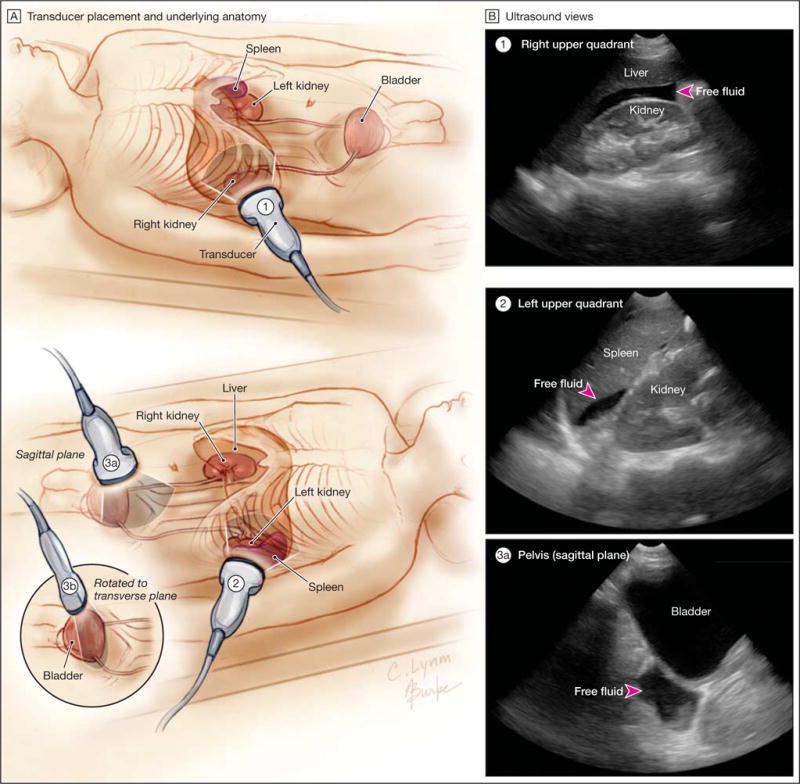
Data synthesis: The prevalence of intra-abdominal injury in adult emergency department patients with blunt abdominal trauma among all evidence level 1 and 2 studies was 13% (95% CI, 10%-17%), with 4.7% (95% CI, 2.5%-8.6%) requiring therapeutic surgery or angiographic embolization of injuries. The presence of a seat belt sign (likelihood ratio [LR] range, 5.6-9.9), rebound tenderness (LR, 6.5; 95% CI, 1.8-24), hypotension (LR, 5.2; 95% CI, 3.5-7.5), abdominal distention (LR, 3.8; 95% CI, 1.9-7.6), or guarding (LR, 3.7; 95% CI, 2.3-5.9) suggest an intra-abdominal injury. The absence of abdominal tenderness to palpation does not rule out an intra-abdominal injury (summary LR, 0.61; 95% CI, 0.46-0.80). The presence of intraperitoneal fluid or organ injury on bedside ultrasound assessment is more accurate than any history and physical examination findings (adjusted summary LR, 30; 95% CI, 20-46); conversely, a normal ultrasound result decreases the chance of injury detection (adjusted summary LR, 0.26; 95% CI, 0.19-0.34). Test results increasing the likelihood of intra-abdominal injury include a base deficit less than -6 mEq/L (LR, 18; 95% CI, 11-30), elevated liver transaminases (LR range, 2.5-5.2), hematuria (LR range, 3.7-4.1), anemia (LR range, 2.2-3.3), and abnormal chest radiograph (LR range, 2.5-3.8). Symptoms and signs may be most useful in combination, particularly in identification of patients who do not need further diagnostic workup.
Conclusions: Bedside ultrasonography has the highest accuracy of all individual findings, but a normal result does not rule out an intra-abdominal injury. Combinations of clinical findings may be most useful to determine which patients do not require further evaluation, but the ideal combination of variables for identifying patients without intra-abdominal injury requires further study.
Conflict of interest statement
Figures

Comment in
-
ACP Journal Club: review: bedside ultrasonography has 82% sensitivity and 99% specificity for blunt intraabdominal injury.Ann Intern Med. 2012 Aug 21;157(4):JC2-12. doi: 10.7326/0003-4819-157-4-201208210-02012. Ann Intern Med. 2012. PMID: 22910966 No abstract available.
-
How useful are clinical findings in patients with blunt abdominal trauma?Ann Emerg Med. 2014 Apr;63(4):463-4. doi: 10.1016/j.annemergmed.2013.03.028. Epub 2013 May 23. Ann Emerg Med. 2014. PMID: 23706748 No abstract available.
References
-
- Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, Tejada-Vera B. Deaths: final data for 2006. Natl Vital Stat Rep. 2009;57(14):1–134. - PubMed
-
- Isenhour JL, Marx J. Advances in abdominal trauma. Emerg Med Clin North Am. 2007;25(3):713–733. - PubMed
-
- Fakhry SM, Brownstein M, Watts DD, Baker CC, Oller D. Relatively short diagnostic delays (<8 hours) produce morbidity and mortality in blunt small bowel injury: an analysis of time to operative intervention in 198 patients from a multicenter experience. J Trauma. 2000;48(3):408–414. discussion 414–415. - PubMed
-
- Niederee MJ, Byrnes MC, Helmer SD, Smith RS. Delay in diagnosis of hollow viscus injuries: effect on outcome. Am Surg. 2003;69(4):293–298. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
