

Expanding the spectrum of monoclonal light chain deposition disease in muscle
- PMID: 22499107
- PMCID: PMC4133774
- DOI: 10.1002/mus.23287
Expanding the spectrum of monoclonal light chain deposition disease in muscle
Abstract
Introduction: The diagnosis of amyloid myopathy is delayed when monoclonal gammopathies are not detected on initial testing and muscle biopsies are nondiagnostic, and the EMG and symptoms can mimic an inflammatory myopathy.
Methods: Case report of a patient presenting with severe progressive muscle weakness of unclear etiology despite an extensive workup including two nondiagnostic muscle biopsies.
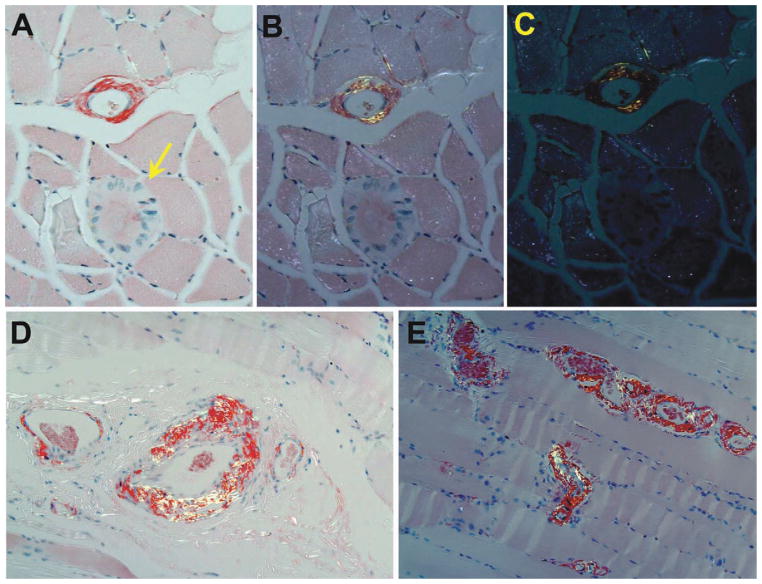
Results: Directed by MRI, a third biopsy revealed amyloid angiopathy and noncongophilic kappa light chain deposition in scattered subsarcolemmal rings and perimysial regions. A serum free light chain (FLC) assay revealed a kappa monoclonal gammopathy, which was not detected by multiple immunofixations.
Conclusions: The spectrum of immunoglobulin deposition in muscle is similar to other organs. It comprises a continuum that includes parenchymal amyloid deposition, amyloid angiopathy, and noncongophilic Light Chain Deposition Disease (LCDD). We recommend including the FLC assay in the routine investigation for monoclonal gammopathies. This case also highlights the value of MRI-guided muscle biopsy.
Copyright © 2012 Wiley Periodicals, Inc.
Figures



References
-
- Nadkarni N, Freimer M, Mendell JR. Amyloidosis causing a progressive myopathy. Muscle Nerve. 1995;18:1016–1018. - PubMed
-
- Chapin JE, Kornfeld M, Harris A. Amyloid myopathy: characteristic features of a still underdiagnosed disease. Muscle Nerve. 2005;31:266–272. - PubMed
-
- Metzler JP, Fleckenstein JL, White CL, Haller RG, Frenkel EP, Greenlee RG. MRI evaluation of amyloid myopathy. Skeletal Radiol. 1992;21:463–465. - PubMed
-
- Ganeval D, Noel LH, Preud’homme JL, Droz D, Grunfeld JP. Light-chain deposition disease: its relation with AL-type amyloidosis. Kidney Int. 1984;26:1–9. - PubMed
-
- Kaplan B, Ramirez-Alvarado M, Sikkink L, Golderman S, Dispenzieri A, Livneh A, et al. Free light chains in plasma of patients with light chain amyloidosis and non-amyloid light chain deposition disease. High proportion and heterogeneity of disulfide-linked monoclonal free light chains as pathogenic features of amyloid disease. Br J Haematol. 2009;144:705–715. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
