

A grading system combining architectural features and mitotic count predicts recurrence in stage I lung adenocarcinoma
- PMID: 22499226
- PMCID: PMC4382749
- DOI: 10.1038/modpathol.2012.58
A grading system combining architectural features and mitotic count predicts recurrence in stage I lung adenocarcinoma
Abstract
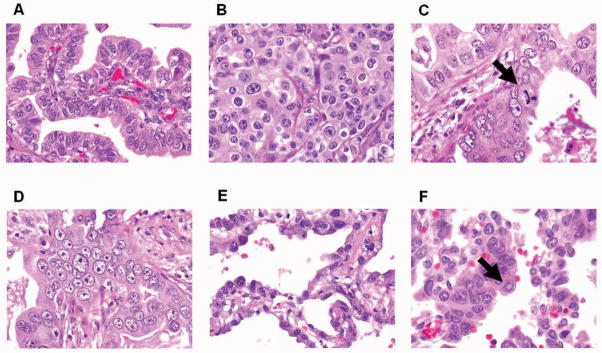
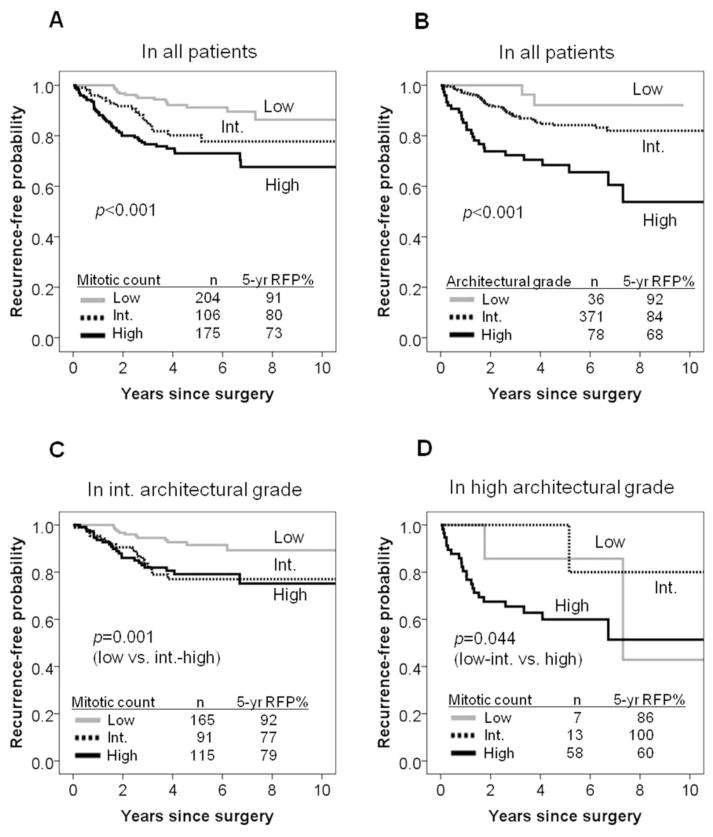
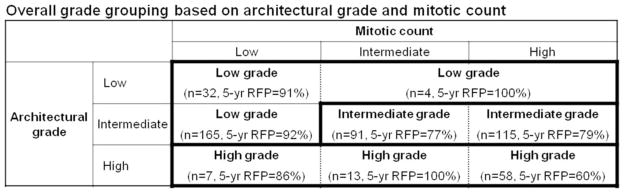
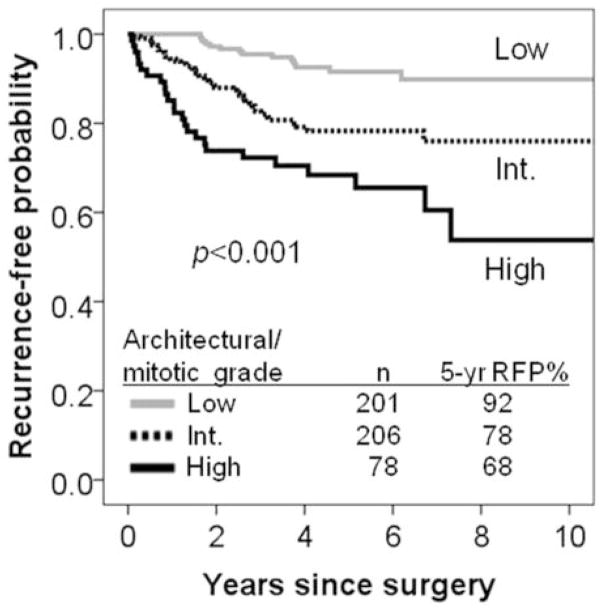
The International Association for the Study of Lung Cancer (IASLC)/American Thoracic Society (ATS)/European Respiratory Society (ERS) has recently proposed a new lung adenocarcinoma classification. We investigated whether nuclear features can stratify prognostic subsets. Slides of 485 stage I lung adenocarcinoma patients were reviewed. We evaluated nuclear diameter, nuclear atypia, nuclear/cytoplasmic ratio, chromatin pattern, prominence of nucleoli, intranuclear inclusions, mitotic count/10 high-power fields (HPFs) or 2.4 mm(2), and atypical mitoses. Tumors were classified into histologic subtypes according to the IASLC/ATS/ERS classification and grouped by architectural grade into low (adenocarcinoma in situ, minimally invasive adenocarcinoma, or lepidic predominant), intermediate (papillary or acinar), and high (micropapillary or solid). Log-rank tests and Cox regression models evaluated the ability of clinicopathologic factors to predict recurrence-free probability. In univariate analyses, nuclear diameter (P=0.007), nuclear atypia (P=0.006), mitotic count (P<0.001), and atypical mitoses (P<0.001) were significant predictors of recurrence. The recurrence-free probability of patients with high mitotic count (≥5/10 HPF: n=175) was the lowest (5-year recurrence-free probability=73%), followed by intermediate (2-4/10 HPF: n=106, 80%), and low (0-1/10 HPF: n=204, 91%, P<0.001). Combined architectural/mitotic grading system stratified patient outcomes (P<0.001): low grade (low architectural grade with any mitotic count and intermediate architectural grade with low mitotic count: n=201, 5-year recurrence-free probability=92%), intermediate grade (intermediate architectural grade with intermediate-high mitotic counts: n=206, 78%), and high grade (high architectural grade with any mitotic count: n=78, 68%). The advantage of adding mitotic count to architectural grade is in stratifying patients with intermediate architectural grade into two prognostically distinct categories (P=0.001). After adjusting for clinicopathologic factors including sex, stage, pleural/lymphovascular invasion, and necrosis, mitotic count was not an independent predictor of recurrence (P=0.178). However, patients with the high architectural/mitotic grade remained at significantly increased risk of recurrence (high vs low: P=0.005) after adjusting for clinical factors. We proposed this combined architectural/mitotic grade for lung adenocarcinoma as a practical method that can be applied in routine practice.
Conflict of interest statement
All authors affirm that we have no actual or potential conflict of interest including any financial, personal or other relationships with other people or organizations.
Figures
References
-
- Devesa SS, Bray F, Vizcaino AP, Parkin DM. International lung cancer trends by histologic type: male:female differences diminishing and adenocarcinoma rates rising. Int J Cancer. 2005;117:294–9. - PubMed
-
- Motoi N, Szoke J, Riely GJ, et al. Lung adenocarcinoma: modification of the 2004 WHO mixed subtype to include the major histologic subtype suggests correlations between papillary and micropapillary adenocarcinoma subtypes, EGFR mutations and gene expression analysis. Am J Surg Pathol. 2008;32:810–27. - PubMed
-
- Okudela K, Woo T, Mitsui H, et al. Morphometric profiling of lung cancers. Its association with clinicopathologic, biologic, and molecular genetic features. Am J Surg Pathol. 2010;34:243–55. - PubMed
-
- Sica G, Yoshizawa A, Sima CS, et al. A grading system of lung adenocarcinomas based on histologic pattern is predictive of disease recurrence in stage I tumors. Am J Surg Pathol. 2010;34(8):1155–62. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
