

Glioblastoma following radiosurgery for meningioma
- PMID: 22500202
- PMCID: PMC3322216
- DOI: 10.3340/jkns.2012.51.2.98
Glioblastoma following radiosurgery for meningioma
Abstract
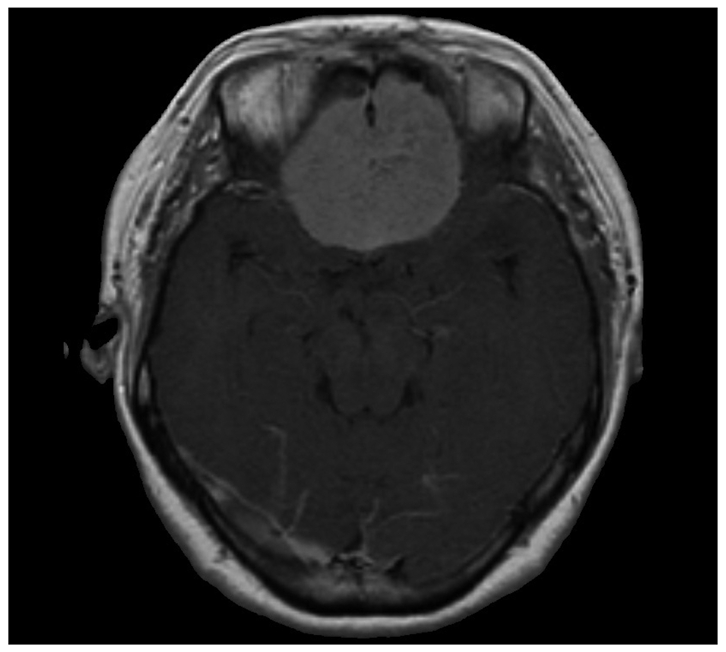
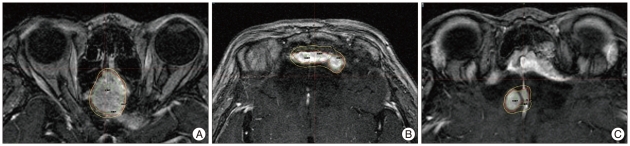
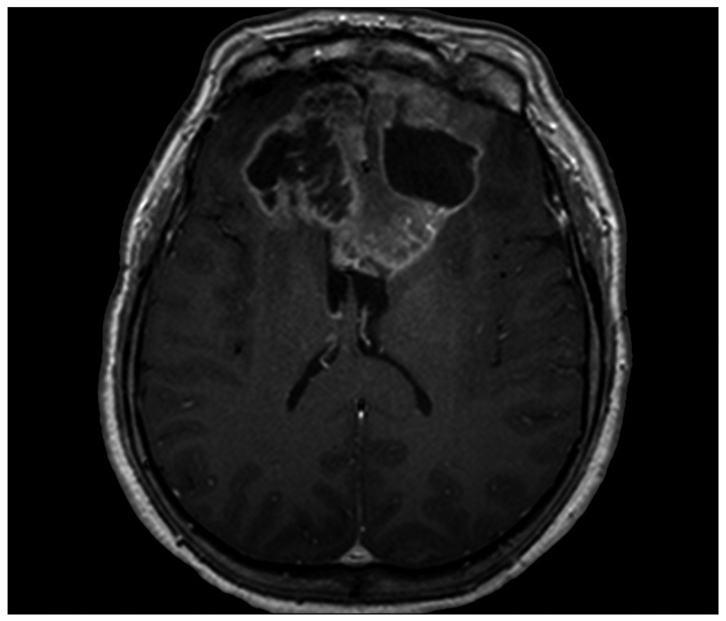
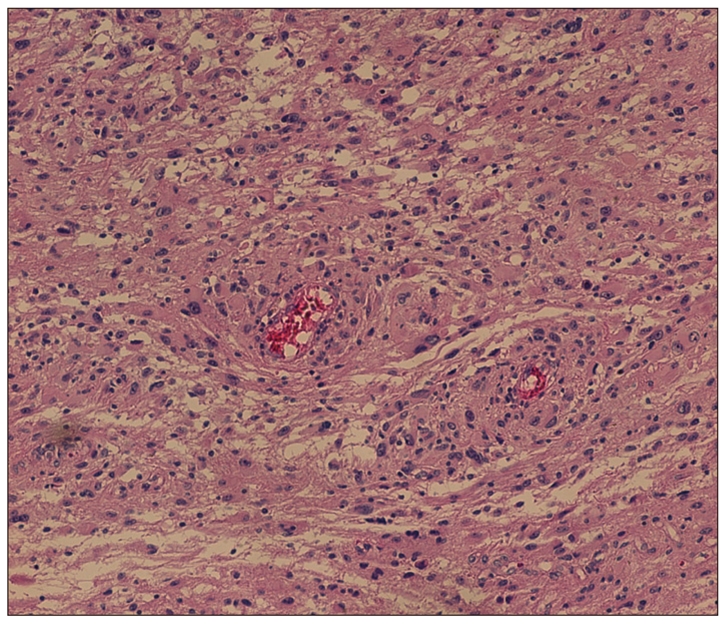
We report a patient who underwent gamma knife radiosurgery to treat recurrent meningioma after microsurgery and thereafter developed secondary malignancy adjacent to the original tumor. A 47-year-old woman had underwent resection of the olfactory groove meningioma. Then radiosurgery was done three times over 4 year period for the recurrent tumor. After 58 months from the initial radiosurgery, she presented with headache and progressive mental dullness. Huge tumor in bifrontal location was revealed in MRI. Subsequent operation and pathological examination confirmed diagnosis of glioblastoma. This case fits the criteria of radiation-induced tumor and the clinical implication of the issue is discussed.
Keywords: Glioblastoma; Radiosurgery.
Figures
References
-
- Bari ME, Forster DM, Kemeny AA, Walton L, Hardy D, Anderson JR. Malignancy in a vestibular schwannoma. Report of a case with central neurofibromatosis, treated by both stereotactic radiosurgery and surgical excision, with a review of the literature. Br J Neurosurg. 2002;16:284–289. - PubMed
-
- Bliss P, Kerr GR, Gregor A. Incidence of second brain tumours after pituitary irradiation in Edinburgh 1962-1990. Clin Oncol (R Coll Radiol) 1994;6:361–363. - PubMed
-
- Boice JD, Jr, Land CE, Shore RE, Norman JE, Tokunaga M. Risk of breast cancer following low-dose radiation exposure. Radiology. 1979;131:589–597. - PubMed
-
- Cahan WG. Radiation-induced sarcoma--50 years later. Cancer. 1998;82:6–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
