

Cardiovascular disease risk factor patterns and their implications for intervention strategies in Vietnam
- PMID: 22500217
- PMCID: PMC3303616
- DOI: 10.1155/2012/560397
Cardiovascular disease risk factor patterns and their implications for intervention strategies in Vietnam
Abstract
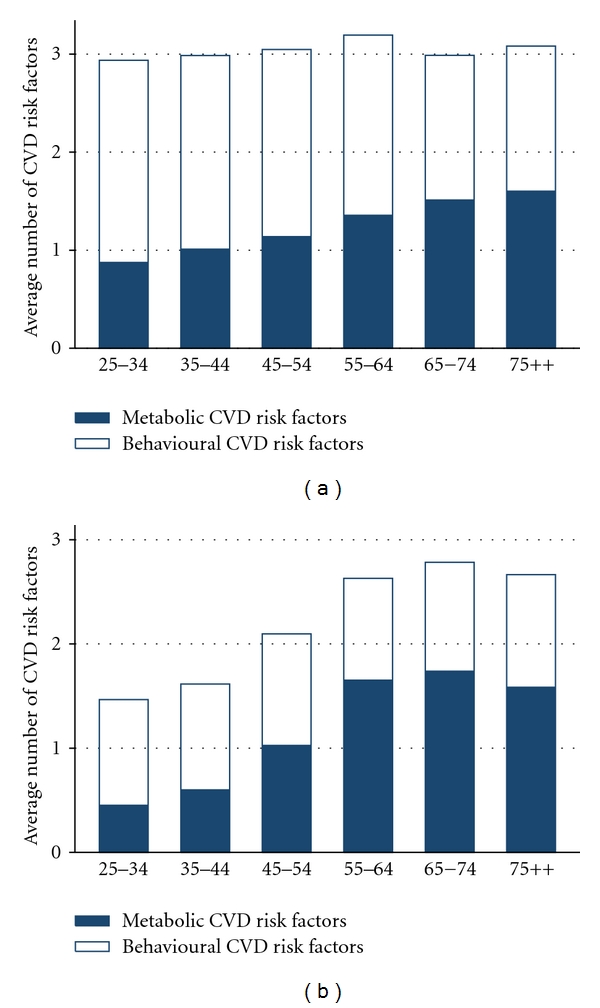
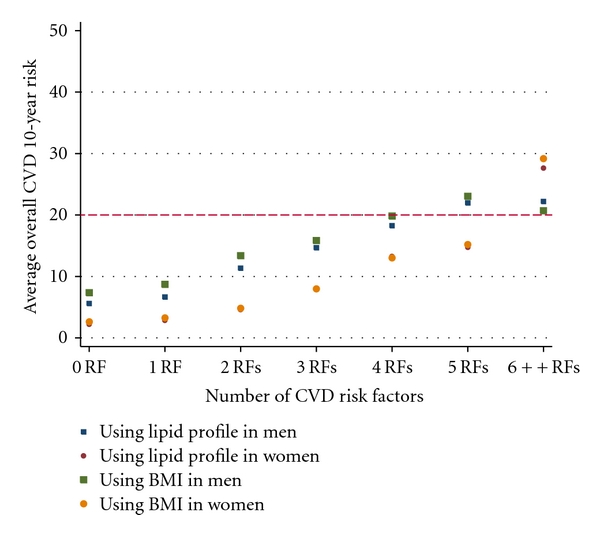
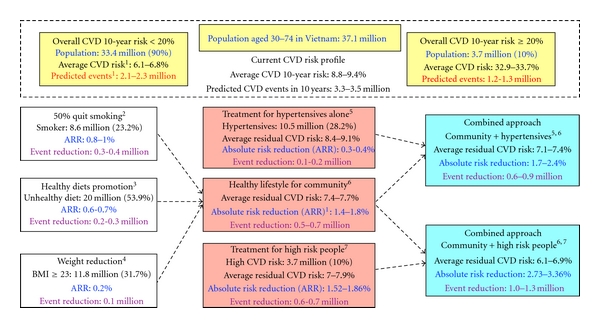
Background. Data on cardiovascular disease risk factors (CVDRFs) in Vietnam are limited. This study explores the prevalence of each CVDRF and how they cluster to evaluate CVDRF burdens and potential prevention strategies. Methods. A cross-sectional survey in 2009 (2,130 adults) was done to collect data on behavioural CVDRF, anthropometry and blood pressure, lipidaemia profiles, and oral glucose tolerance tests. Four metabolic CVDRFs (hypertension, dyslipidaemia, diabetes, and obesity) and five behavioural CVDRFs (smoking, excessive alcohol intake, unhealthy diet, physical inactivity, and stress) were analysed to identify their prevalence, cluster patterns, and social predictors. Framingham scores were applied to estimate the global 10-year CVD risks and potential benefits of CVD prevention strategies. Results. The age-standardised prevalence of having at least 2/4 metabolic, 2/5 behavioural, or 4/9 major CVDRF was 28%, 27%, 13% in women and 32%, 62%, 34% in men. Within-individual clustering of metabolic factors was more common among older women and in urban areas. High overall CVD risk (≥20% over 10 years) identified 20% of men and 5% of women-especially at higher ages-who had coexisting CVDRF. Conclusion. Multiple CVDRFs were common in Vietnamese adults with different clustering patterns across sex/age groups. Tackling any single risk factor would not be efficient.
Figures
References
-
- Yusuf S, Reddy S, Ôunpuu S, Anand S. Global burden of cardiovascular diseases—part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation. 2001;104(22):2746–2753. - PubMed
-
- Feigin VL, Lawes CM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. The Lancet Neurology. 2009;8(4):355–369. - PubMed
-
- Minh HV, Byass P, Wall S. Mortality from cardiovascular diseases in Bavi District, Vietnam. Scandinavian Journal of Public Health. 2003;62:26–31. - PubMed
-
- Vietnam Ministry of Health. Vietnam Health Statistics Yearbook. Vietnam Ministry of Health; 2005.
LinkOut - more resources
Full Text Sources
