

GnRH agonist versus GnRH antagonist in in vitro fertilization and embryo transfer (IVF/ET)
- PMID: 22500852
- PMCID: PMC3442989
- DOI: 10.1186/1477-7827-10-26
GnRH agonist versus GnRH antagonist in in vitro fertilization and embryo transfer (IVF/ET)
Abstract
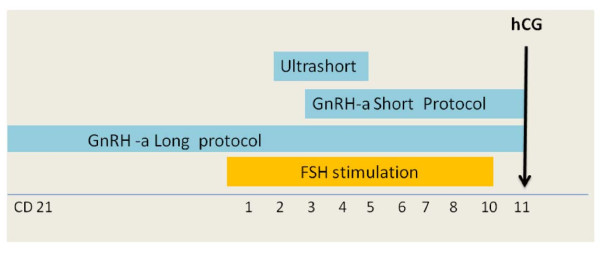
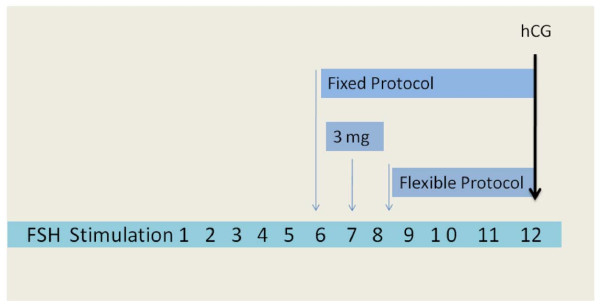
Several protocols are actually available for in Vitro Fertilization and Embryo Transfer. The review summarizes the main differences and the clinic characteristics of the protocols in use with GnRH agonists and GnRH antagonists by emphasizing the major outcomes and hormonal changes associated with each protocol. The majority of randomized clinical trials clearly shows that in "in Vitro" Fertilization and Embryo Transfer, the combination of exogenous Gonadotropin plus a Gonadotropin Releasing Hormone (GnRH) agonist, which is able to suppress pituitary FSH and LH secretion, is associated with increased pregnancy rate as compared with the use of gonadotropins without a GnRH agonist. Protocols with GnRH antagonists are effective in preventing a premature rise of LH and induce a shorter and more cost-effective ovarian stimulation compared to the long agonist protocol. However, a different synchronization of follicular recruitment and growth occurs with GnRH agonists than with GnRH antagonists. Future developments have to be focused on timing of the administration of GnRH antagonists, by giving a great attention to new strategies of stimulation in patients in which radio-chemotherapy cycles are needed.
Figures
References
-
- Caspi E, Ron-El R, Golan A, Nachum H, Herman A, Soffer Y, Weinraub Z. Results of in vitro fertilization and embryo transfer by combined long-acting gonadotropin-releasing hormone analog D-Trp-6-luteinizing hormone-releasing hormone and gonadotropins. Fertil Steril. 1989;51(1):95–99. - PubMed
-
- Liu HC, Lai YM, Davis O, Berkeley AS, Graf M, Grifo J, Cohen J, Rosenwaks Z. Improved pregnancy outcome with gonadotropin releasing hormone agonist (GnRH-a) stimulation is due to the improvement in oocyte quantity rather than quality. J Assist Reprod Genet. 1992;9(4):338–344. doi: 10.1007/BF01203956. - DOI - PubMed
-
- Zorn JR, Boyer P, Guichard A. Never on a Sunday: programming for IVF-ET and GIFT. Lancet. 1987;1(8529):385–386. - PubMed
-
- Daya S. Gonadotropin releasing hormone agonist protocols for pituitary desensitization in in vitro fertilization and gamete intrafallopian transfer cycles. Cochrane Database Syst Rev. 2000;2:CD001299. - PubMed
-
- Albuquerque LE, Saconato H, Maciel MC. Depot versus daily administration of gonadotrophin releasing hormone agonist protocols for pituitary desensitization in assisted reproduction cycles. Cochrane Database Syst Rev. 2005;1:CD002808. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
