

Serum cortisol predicts death and critical disease independently of CRB-65 score in community-acquired pneumonia: a prospective observational cohort study
- PMID: 22501026
- PMCID: PMC3353228
- DOI: 10.1186/1471-2334-12-90
Serum cortisol predicts death and critical disease independently of CRB-65 score in community-acquired pneumonia: a prospective observational cohort study
Abstract
Background: Several biomarkers and prognostic scores have been evaluated to predict prognosis in community-acquired pneumonia (CAP). Optimal risk stratification remains to be evaluated. The aim of this study was to evaluate serum cortisol as biomarker for the prediction of adverse outcomes independently of the CRB-65 score und inflammatory biomarkers in a large cohort of hospitalised patients with CAP.
Methods: 984 hospitalised CAP-patients were included. Serum cortisol was measured and its prognostic accuracy compared to the CRB-65 score, leucocyte count and C-reactive protein. Predefined endpoints were 30-day mortality and the combined endpoint critical pneumonia, defined as presence of death occurring during antibiotic treatment, mechanical ventilation, catecholamine treatment or ICU admission.
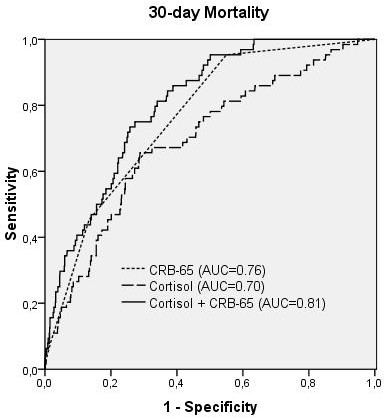
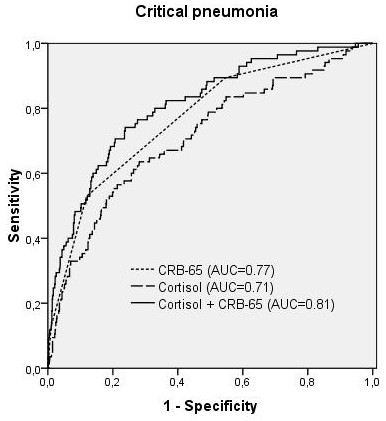
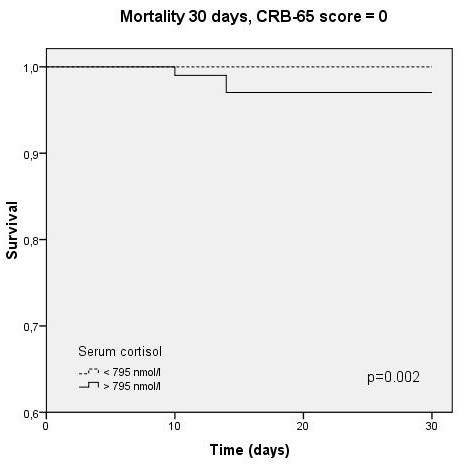
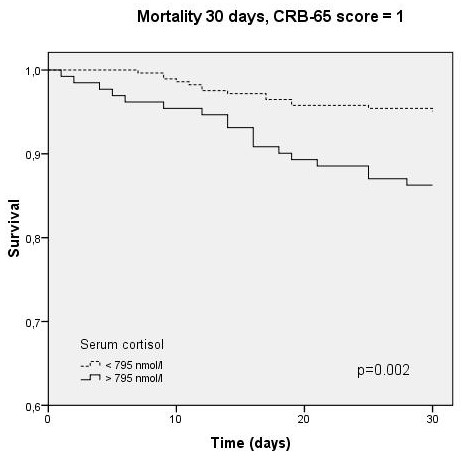
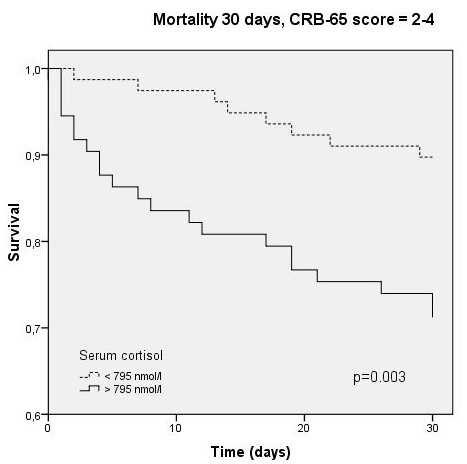
Results: 64 patients died (6.5%) and 85 developed critical pneumonia (8.6%). Cortisol levels were significantly elevated in both adverse outcomes (p < 0.001) and predicted mortality (AUC 0.70, cut-off 795 nmol/L) and critical pneumonia (AUC 0.71) independently of all other measured variables after logistic regression analysis (p = 0.005 and 0.001, respectively). Prognostic accuracy of CRB-65 was significantly improved by adding cortisol levels (combined AUC 0.81 for both endpoints). In Kaplan-Meier analysis, cortisol predicted survival within different CRB-65 strata (p = 0.003). In subgroup analyses, cortisol independently predicted critical pneumonia when compared to procalcitonin, the CURB65 score and minor criteria for severe pneumonia according to the 2007 ATS/IDSA-guideline.
Conclusion: Cortisol predicts mortality and critical disease in hospitalised CAP-patients independently of clinical scores and inflammatory biomarkers. It should be incorporated into trials assessing optimal combinations of clinical criteria and biomarkers to improve initial high risk prediction in CAP.
Figures


References
-
- Chalmers JD, Singanayagam A, Akram AR, Mandal P, Short PM, Choudhury G, Wood V, Hill AT. Severity assessment tools for predicting mortality in hospitalised patients with community-acquired pneumonia. Systematic review and meta-analysis. Thorax. 2010;65:878–883. doi: 10.1136/thx.2009.133280. - DOI - PubMed
-
- Höffken G, Lorenz J, Kern W, Welte T, Bauer T, Dalhoff K, Dietrich E, Ewig S, Gastmeier P, Grabein B, Halle E, Kolditz M, Marre R, Sitter H. Epidemiology, diagnosis, antimicrobial therapy and management of community-acquired pneumonia and lower respiratory tract infections in adults. Guidelines of the Paul-Ehrlich-Society for Chemotherapy, the German Respiratory Society, the German Society for Infectiology and the Competence Network CAPNETZ Germany. Pneumologie. 2009;63:e1–e68. doi: 10.1055/s-0029-1215037. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
