

Nutritional modulation of age-related macular degeneration
- PMID: 22503690
- PMCID: PMC3392439
- DOI: 10.1016/j.mam.2012.03.005
Nutritional modulation of age-related macular degeneration
Abstract
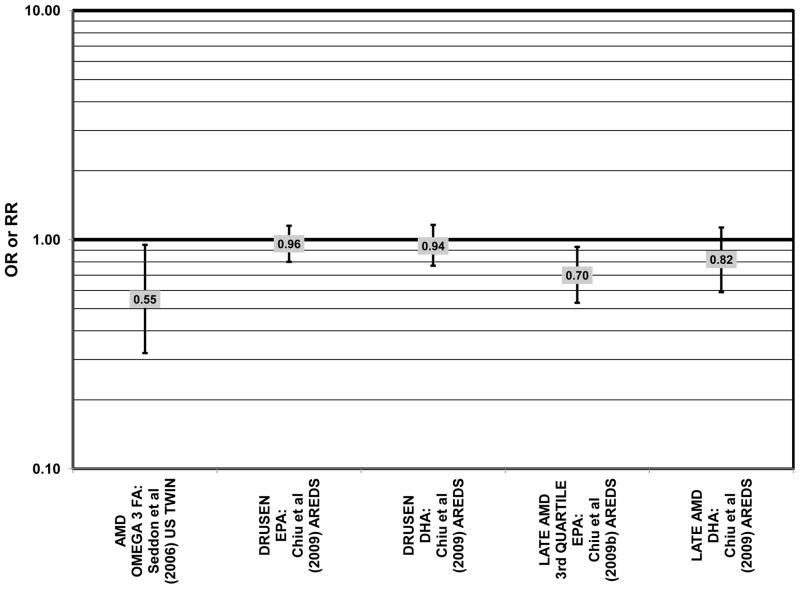
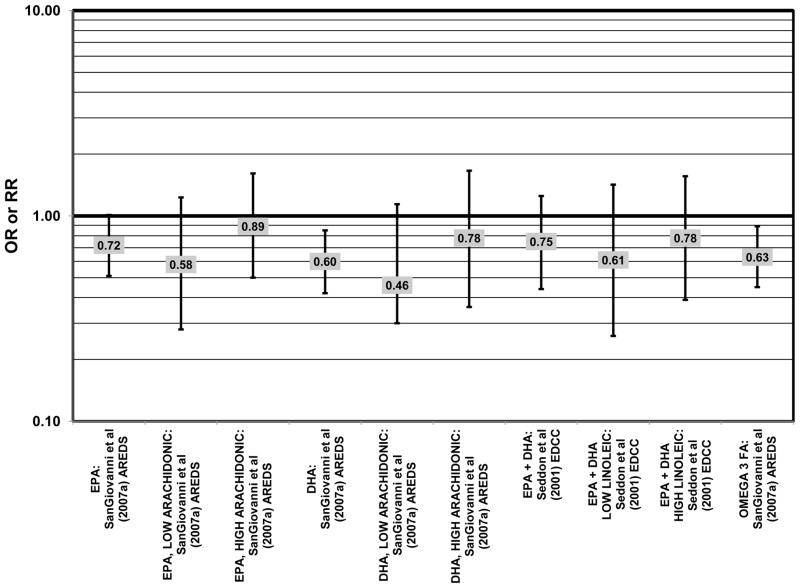
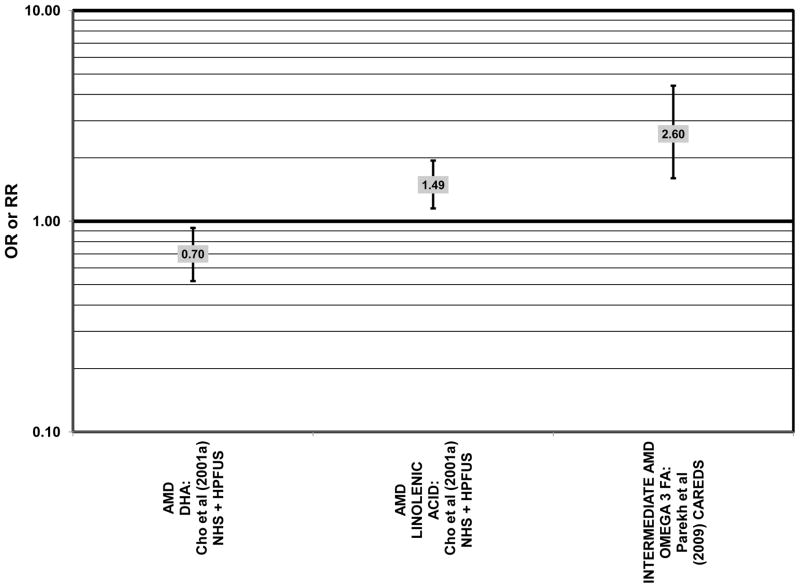
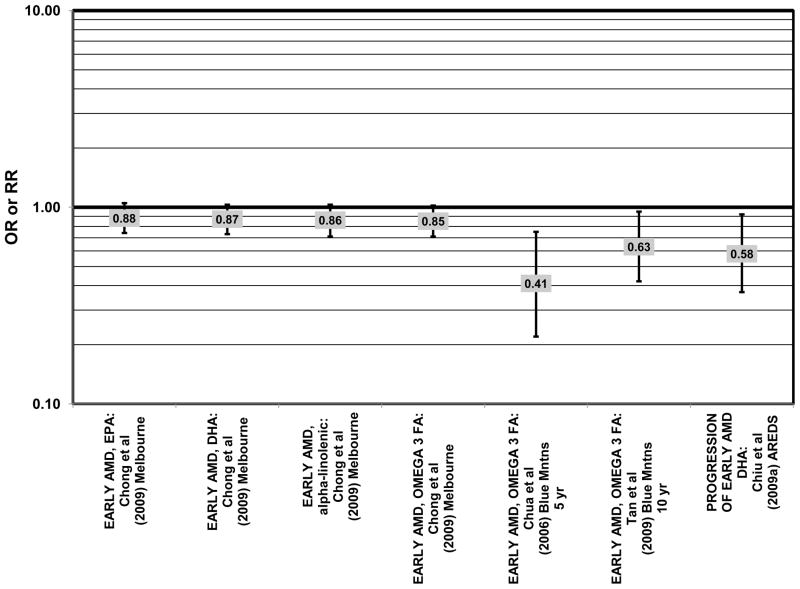
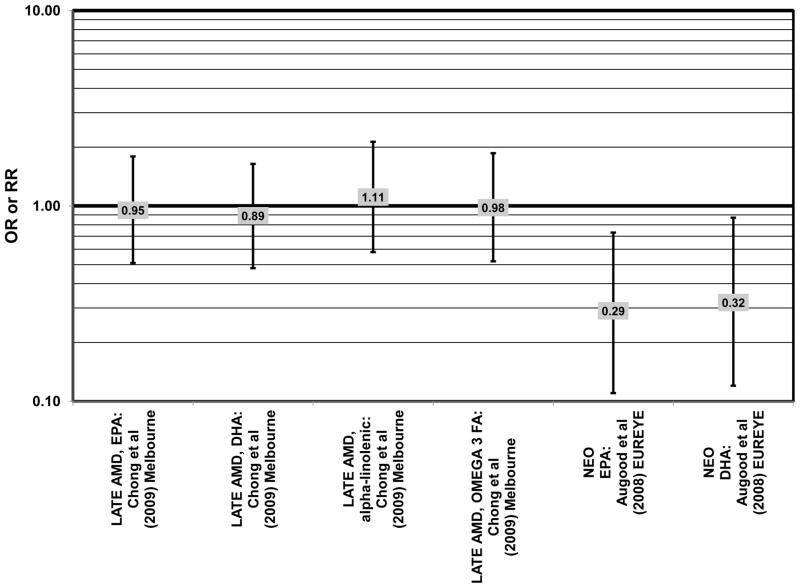
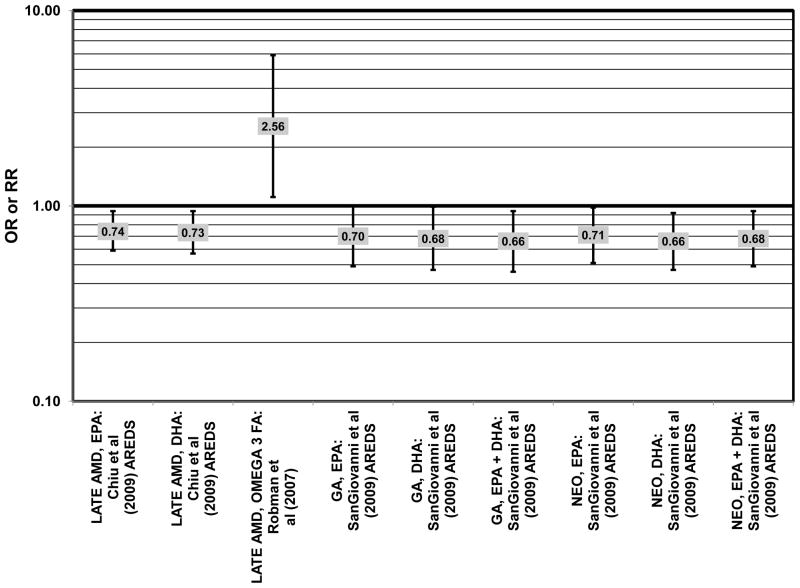
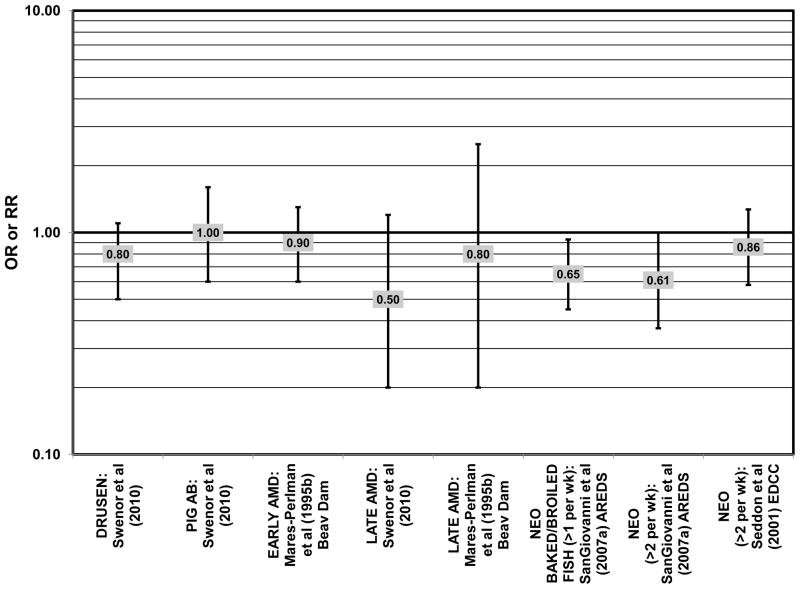
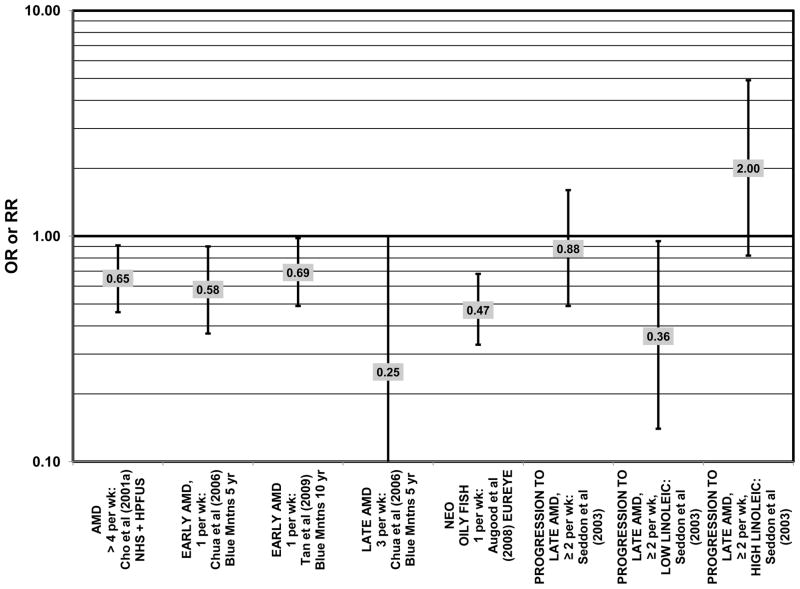
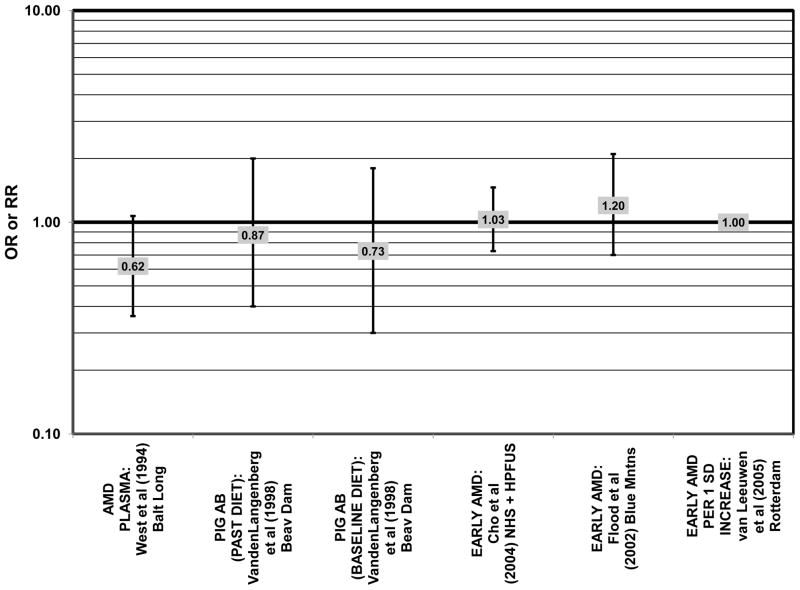
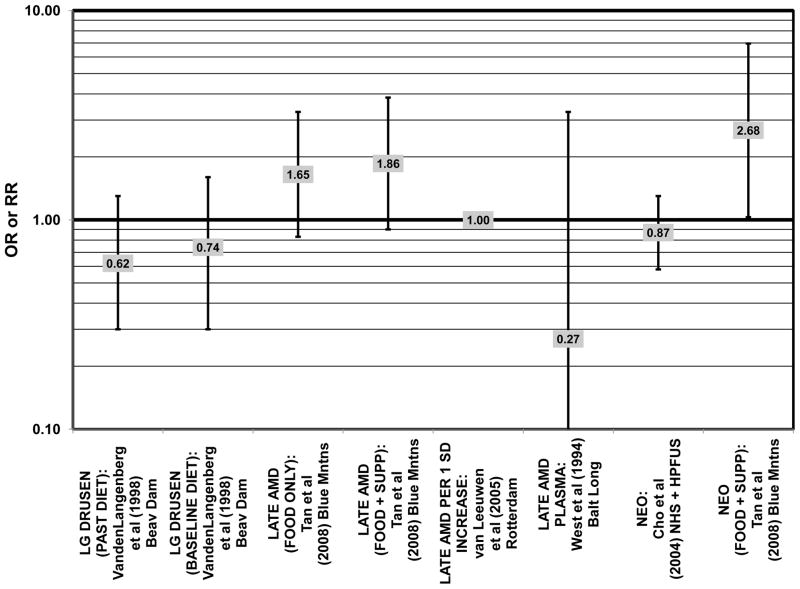
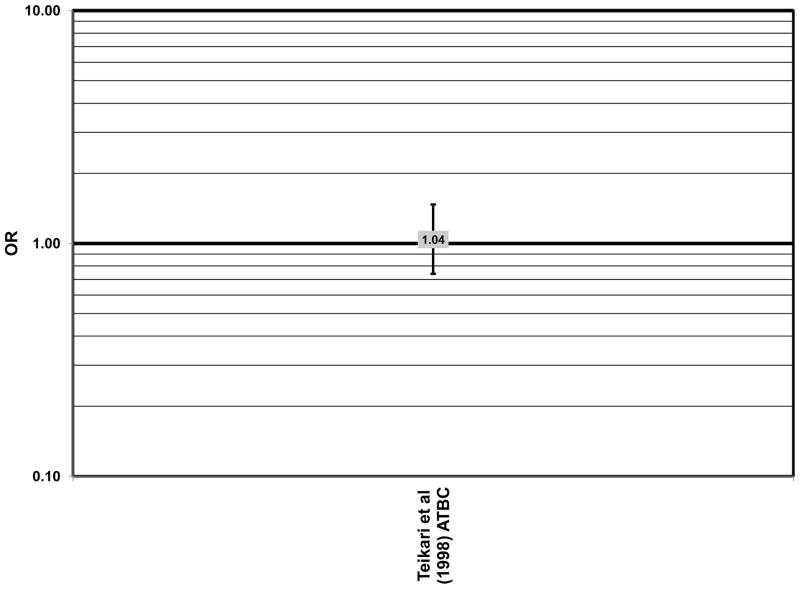
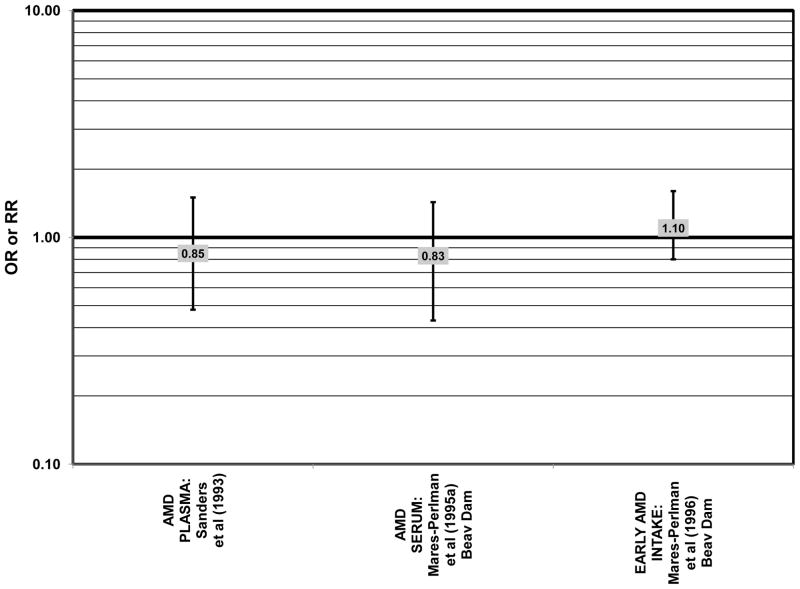
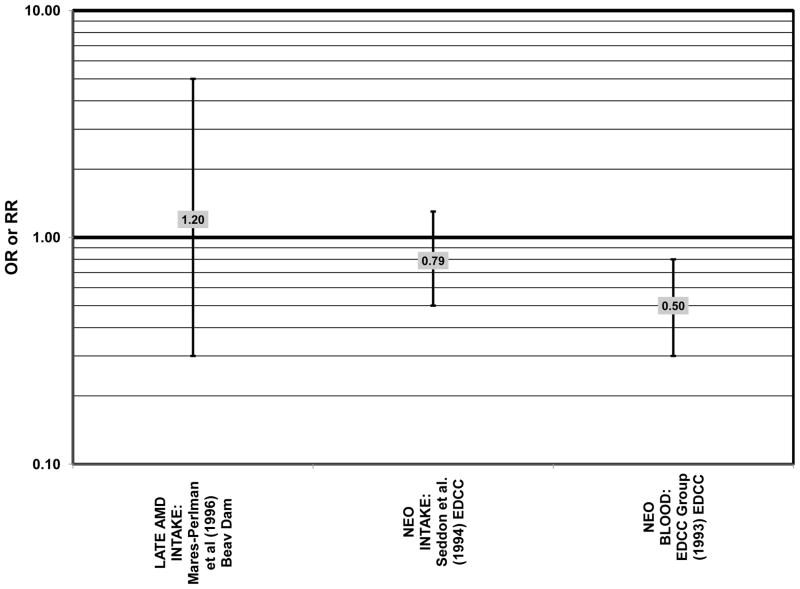
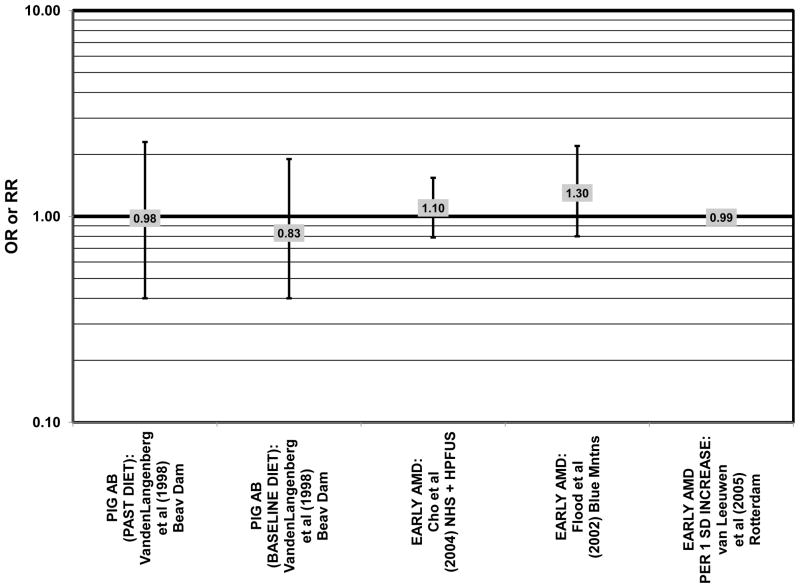
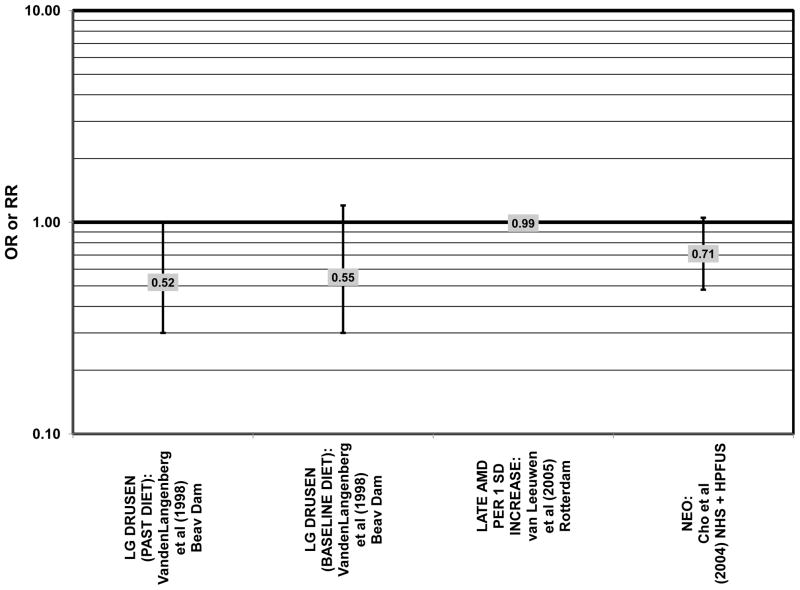
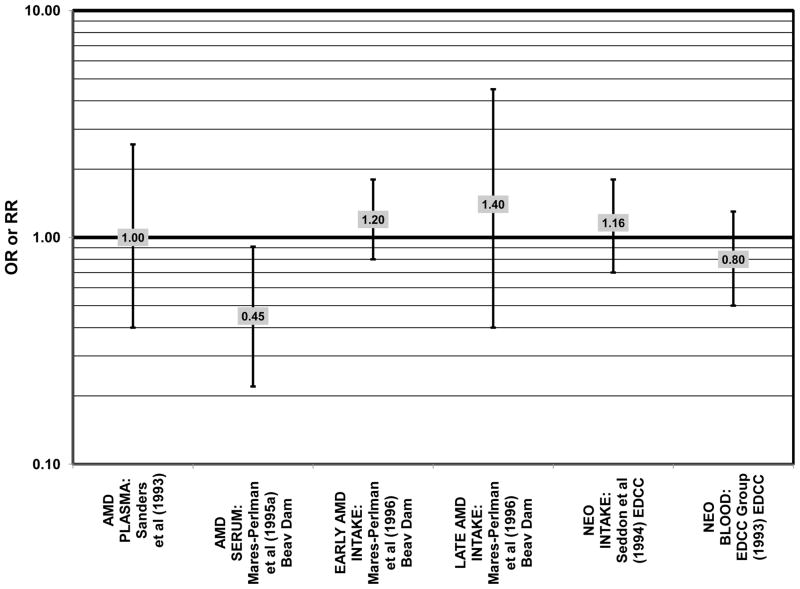
Age-related macular degeneration (AMD) is the leading cause of blindness in the elderly worldwide. It affects 30-50 million individuals and clinical hallmarks of AMD are observed in at least one third of persons over the age of 75 in industrialized countries (Gehrs et al., 2006). Costs associated with AMD are in excess of $340 billion US (American-Health-Assistance-Foundation, 2012). The majority of AMD patients in the United States are not eligible for clinical treatments (Biarnes et al., 2011; Klein et al., 2011). Preventive interventions through dietary modulation are attractive strategies because many studies suggest a benefit of micro- and macronutrients with respect to AMD, as well as other age-related debilities, and with few, if any, adverse effects (Chiu, 2011). Preservation of vision would enhance quality of life for millions of elderly people, and alleviate the personal and public health financial burden of AMD (Frick et al., 2007; Wood et al., 2011). Observational studies indicate that maintaining adequate levels of omega-3 fatty acids (i.e. with 2 servings/week of fish) or a low glycemic index diet may be particularly beneficial for early AMD and that higher levels of carotenoids may be protective, most probably, against neovascular AMD. Intervention trials are needed to better understand the full effect of these nutrients and/or combinations of nutrients on retinal health. Analyses that describe effects of a nutrient on onset and/or progress of AMD are valuable because they indicate the value of a nutrient to arrest AMD at the early stages. This comprehensive summary provides essential information about the value of nutrients with regard to diminishing risk for onset or progress of AMD and can serve as a guide until data from ongoing intervention trials are available.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures




References
-
- Al-Hussaini H, Schneiders M, Lundh P, Jeffery G. Drusen are associated with local and distant disruptions to human retinal pigment epithelium cells. Exp Eye Res. 2009;88 (3):610–612. - PubMed
-
- Allikmets R, Shroyer NF, Singh N, Seddon JM, Lewis RA, Bernstein PS, Peiffer A, Zabriskie NA, Li Y, Hutchinson A, Dean M, Lupski JR, Leppert M. Mutation of the Stargardt disease gene (ABCR) in age-related macular degeneration. Science. 1997;277 (5333):1805–1807. - PubMed
-
- American-Health-Assistance-Foundation. Facts on Macular Degeneration, Macular Degeneration Research. American Health Assistance Foundation; Clarksburg, MD: 2012.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
