

Patellofemoral joint compression forces in backward and forward running
- PMID: 22503882
- PMCID: PMC3391667
- DOI: 10.1016/j.jbiomech.2012.03.020
Patellofemoral joint compression forces in backward and forward running
Abstract
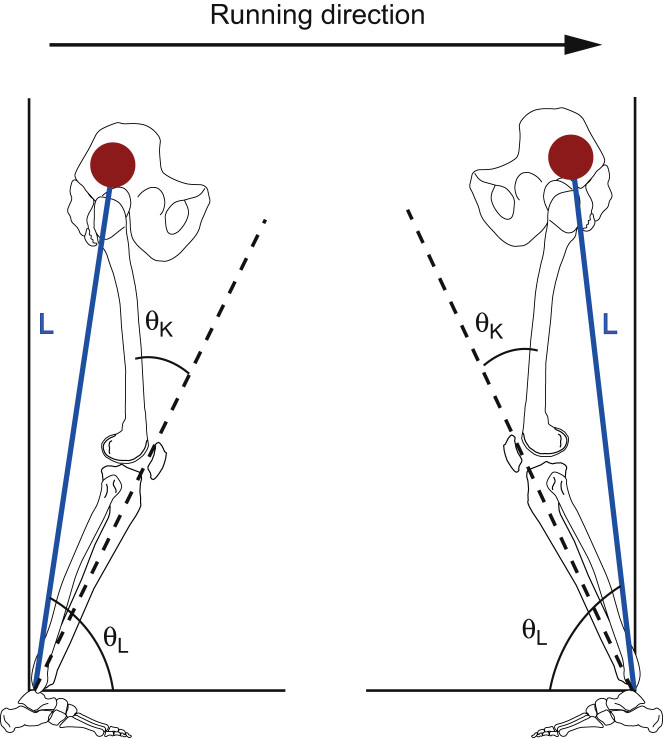
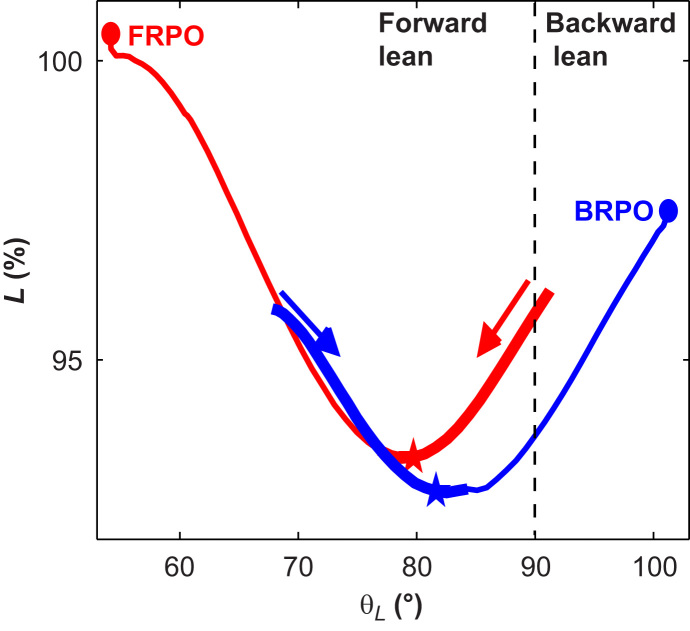
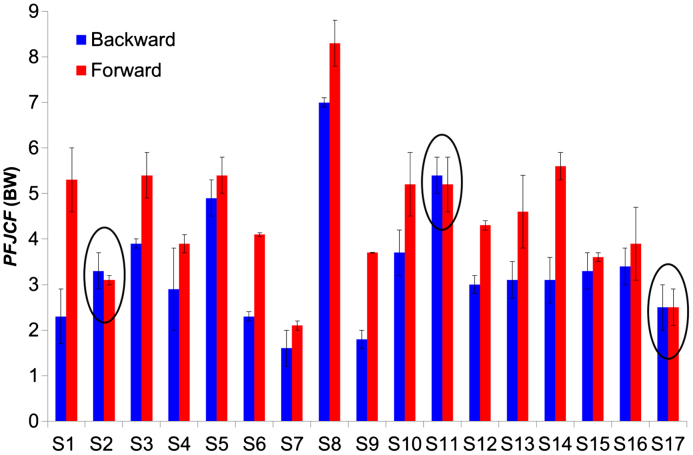
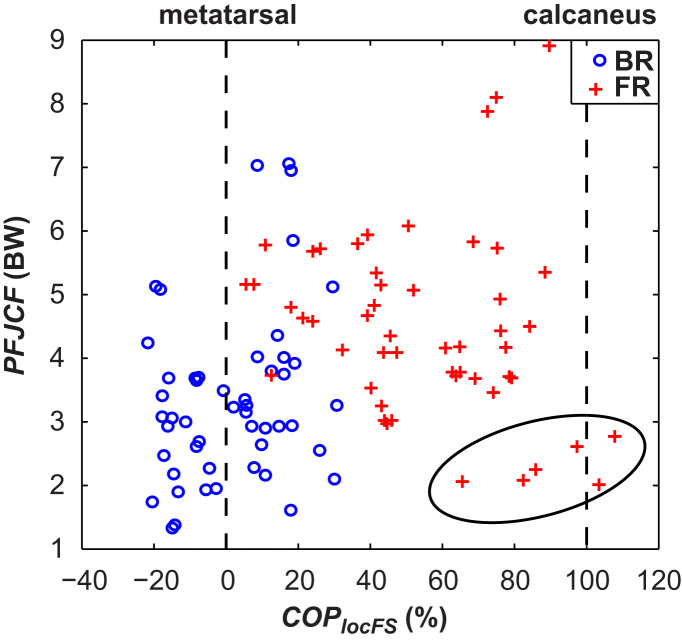
Patellofemoral pain (PFP) is a common injury and increased patellofemoral joint compression forces (PFJCF) may aggravate symptoms. Backward running (BR) has been suggested for exercise with reduced PFJCF. The aims of this study were to (1) investigate if BR had reduced peak PFJCF compared to forward running (FR) at the same speed, and (2) if PFJCF was reduced in BR, to investigate which biomechanical parameters explained this. It was hypothesized that (1) PFJCF would be lower in BR, and (2) that this would coincide with a reduced peak knee moment caused by altered ground reaction forces (GRFs). Twenty healthy subjects ran in forward and backward directions at consistent speed. Kinematic and ground reaction force data were collected; inverse dynamic and PFJCF analyses were performed. PFJCF were higher in FR than BR (4.5±1.5; 3.4±1.4BW; p<0.01). The majority of this difference (93.1%) was predicted by increased knee moments in FR compared to BR (157±54; 124±51 Nm; p<0.01). 54.8% of differences in knee moments could be predicted by the magnitude of the GRF (2.3±0.3; 2.4±0.2BW), knee flexion angle (44±6; 41±7) and center of pressure location on the foot (25±11; 12±6%) at time of peak knee moment. Results were not consistent in all subjects. It was concluded that BR had reduced PFJCF compared to FR. This was caused by an increased knee moment, due to differences in magnitude and location of the GRF vector relative to the knee. BR can therefore be used to exercise with decreased PFJCF.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
References
-
- Baltzopoulos V. Muscular and tibiofemoral joint forces during isokinetic concentric knee extension. Clinical Biomechechanics. 1995;19:208–214. - PubMed
-
- Besier T.F., Draper C.E., Gold G.E., Beaupré G.S., Delp S.L. Patellofemoral joint contact area increases with knee flexion and weight-bearing. Journal of Orthopaedic Research. 2005;23(2):345–350. - PubMed
-
- Buckwalter J., Brown T. Joint injury, repair, and remodeling. Clinical Orthopaedics and Related Research. 2004;423:7–16. - PubMed
-
- Buford W.L., Ivey F.M., Malone J.D., Patterson R.M., Peare G.L., Nguyen D.K., Stewart A.A. Muscle balance at the knee–moment arms for the normal knee and the ACL-minus knee. IEEE Transactions on Rehabilitation Engineering. 1997;5(4):367–379. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
