

Nuclear morphometry, nucleomics and prostate cancer progression
- PMID: 22504875
- PMCID: PMC3720156
- DOI: 10.1038/aja.2011.148
Nuclear morphometry, nucleomics and prostate cancer progression
Abstract
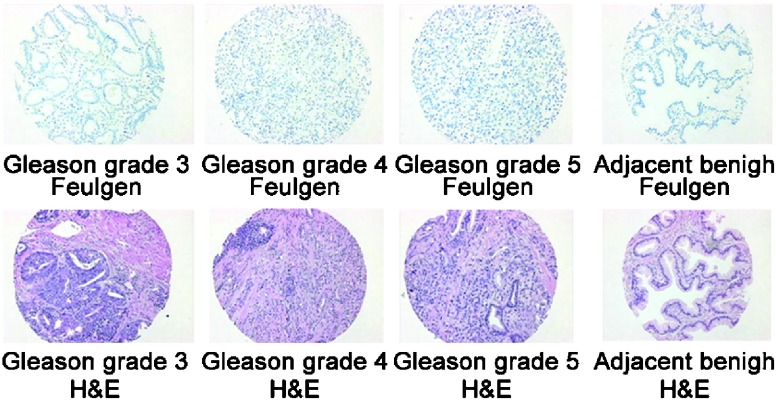
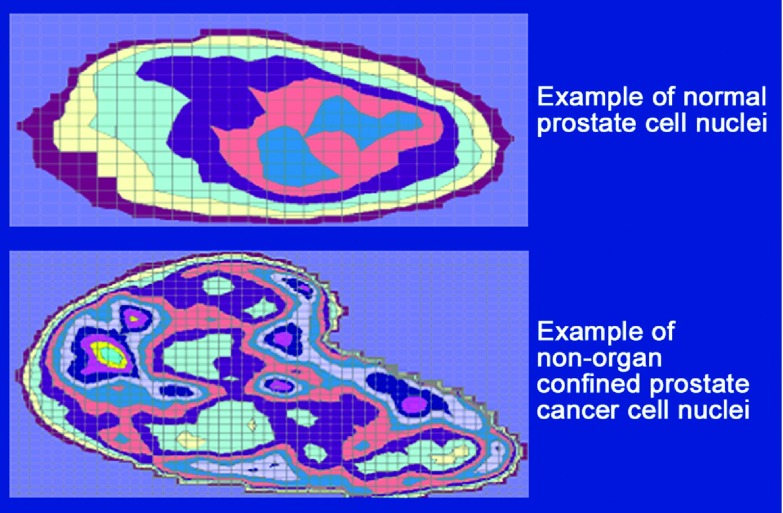
Prostate cancer (PCa) results from a multistep process. This process includes initiation, which occurs through various aging events and multiple insults (such as chronic infection, inflammation and genetic instability through reactive oxygen species causing DNA double-strand breaks), followed by a multistep process of progression. These steps include several genetic and epigenetic alterations, as well as alterations to the chromatin structure, which occur in response to the carcinogenic stress-related events that sustain proliferative signaling. Events such as evading growth suppressors, resisting cell death, enabling replicative immortality, inducing angiogenesis, and activating invasion and metastasis are readily observed. In addition, in conjunction with these critical drivers of carcinogenesis, other factors related to the etiopathogenesis of PCa, involving energy metabolism and evasion of the immune surveillance system, appear to be involved. In addition, when cancer spread and metastasis occur, the 'tumor microenvironment' in the bone of PCa patients may provide a way to sustain dormancy or senescence and eventually establish a 'seed and soil' site where PCa proliferation and growth may occur over time. When PCa is initiated and progression ensues, significant alterations in nuclear size, shape and heterochromatin (DNA transcription) organization are found, and key nuclear transcriptional and structural proteins, as well as multiple nuclear bodies can lead to precancerous and malignant changes. These series of cellular and tissue-related malignancy-associated events can be quantified to assess disease progression and management.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Etzioni R, Penson DF, Legler JM, di Tommaso D, Boer R, et al. Overdiagnosis due to prostate-specific antigen screening: lessons from U.S. prostate cancer incidence trends. J Natl Cancer Inst. 2002;94:981–90. - PubMed
-
- Draisma G, Boer R, Otto SJ, van der Cruijsen IW, Damhuis RA, et al. Lead times and overdetection due to prostate-specific antigen screening: estimates from the European Randomized Study of Screening for Prostate Cancer. J Natl Cancer Inst. 2003;95:868–78. - PubMed
-
- Albertsen PC. Treatment of localized prostate cancer: when is active surveillance appropriate. Nat Rev Clin Oncol. 2010;7:394–400. - PubMed
-
- Bastian PJ, Carter BH, Bjartell A, Seitz M, Stanislaus P, et al. Insignificant prostate cancer and active surveillance: from definition to clinical implications. Eur Urol. 2009;55:1321–30. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
