

A DNA repair pathway-focused score for prediction of outcomes in ovarian cancer treated with platinum-based chemotherapy
- PMID: 22505474
- PMCID: PMC3341307
- DOI: 10.1093/jnci/djs177
A DNA repair pathway-focused score for prediction of outcomes in ovarian cancer treated with platinum-based chemotherapy
Abstract
Background: New tools are needed to predict outcomes of ovarian cancer patients treated with platinum-based chemotherapy. We hypothesized that a molecular score based on expression of genes that are involved in platinum-induced DNA damage repair could provide such prognostic information.
Methods: Gene expression data was extracted from The Cancer Genome Atlas (TCGA) database for 151 DNA repair genes from tumors of serous ovarian cystadenocarcinoma patients (n = 511). A molecular score was generated based on the expression of 23 genes involved in platinum-induced DNA damage repair pathways. Patients were divided into low (scores 0-10) and high (scores 11-20) score groups, and overall survival (OS) was analyzed by Kaplan-Meier method. Results were validated in two gene expression microarray datasets. Association of the score with OS was compared with known clinical factors (age, stage, grade, and extent of surgical debulking) using univariate and multivariable Cox proportional hazards models. Score performance was evaluated by receiver operating characteristic (ROC) curve analysis. Correlations between the score and likelihood of complete response, recurrence-free survival, and progression-free survival were assessed. Statistical tests were two-sided.
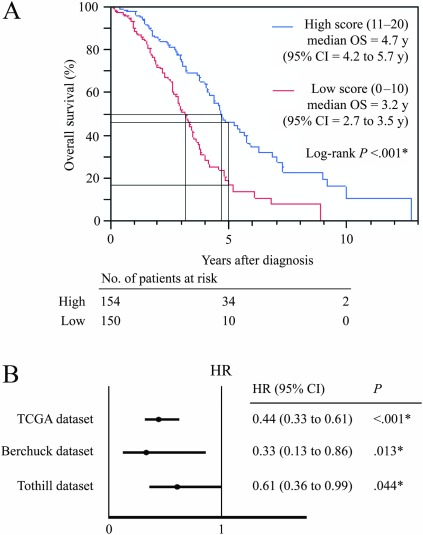
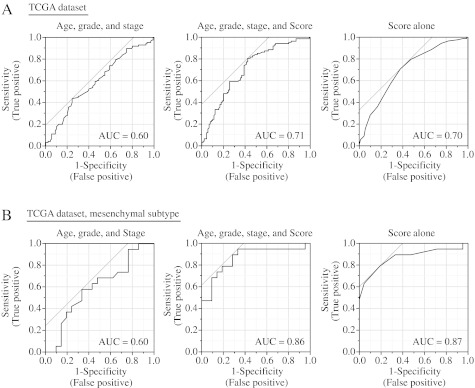
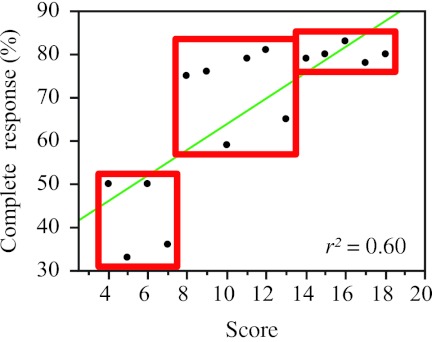
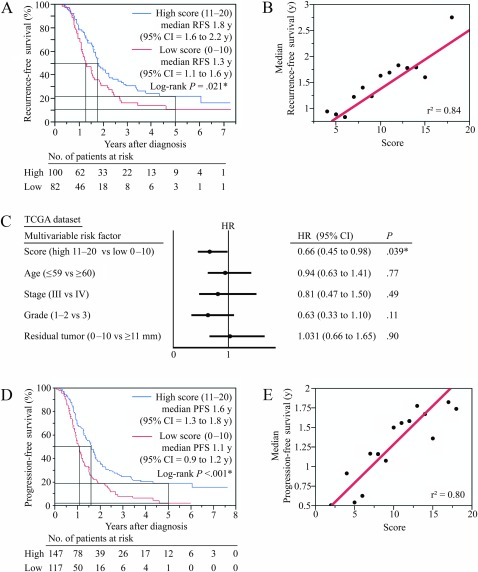
Results: Improved survival was associated with being in the high-scoring group (high vs low scores: 5-year OS, 40% vs 17%, P < .001), and results were reproduced in the validation datasets (P < .05). The score was the only pretreatment factor that showed a statistically significant association with OS (high vs low scores, hazard ratio of death = 0.40, 95% confidence interval = 0.32 to 0.66, P < .001). ROC curves indicated that the score outperformed the known clinical factors (score in a validation dataset vs clinical factors, area under the curve = 0.65 vs 0.52). The score positively correlated with complete response rate, recurrence-free survival, and progression-free survival (Pearson correlation coefficient [r(2)] = 0.60, 0.84, and 0.80, respectively; P < .001 for all).
Conclusion: The DNA repair pathway-focused score can be used to predict outcomes and response to platinum therapy in ovarian cancer patients.
Figures

Comment in
-
Molecular scores to predict ovarian cancer outcomes: a worthy goal, but not ready for prime time.J Natl Cancer Inst. 2012 May 2;104(9):642-5. doi: 10.1093/jnci/djs203. Epub 2012 Apr 13. J Natl Cancer Inst. 2012. PMID: 22505475 Free PMC article. No abstract available.
-
Re: A DNA repair pathway-focused score for prediction of outcomes in ovarian cancer treated with platinum-based chemotherapy.J Natl Cancer Inst. 2012 Oct 3;104(19):1514; author reply 1514-5. doi: 10.1093/jnci/djs363. Epub 2012 Aug 24. J Natl Cancer Inst. 2012. PMID: 22923512 No abstract available.
References
-
- Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA Cancer J Clin. 2010;60(5):277–300. - PubMed
-
- Pignata S, Cannella L, Leopardo D, et al. Chemotherapy in epithelial ovarian cancer. Cancer Lett. 2011;303(2):73–83. - PubMed
-
- Barakat RR, Markman M, Randall ME. Principles and Practice of Gynecologic Oncology. 5 ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009.
-
- Herzog TJ. Clinical experience with topotecan in relapsed ovarian cancer. Gynecol Oncol. 2003;90(3, pt 2):S3–S7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
