

Hypertrophic cranial pachymeningitis and skull base osteomyelitis by pseudomonas aeruginosa: case report and review of the literature
- PMID: 22505989
- PMCID: PMC3320125
- DOI: 10.4021/jocmr777w
Hypertrophic cranial pachymeningitis and skull base osteomyelitis by pseudomonas aeruginosa: case report and review of the literature
Abstract
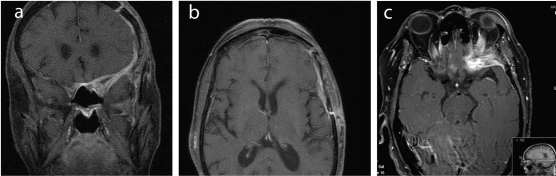
Hypertrophic cranial pachymeningitis (HCP) is an uncommon disorder characterized by localized or diffuse thickening of the dura mater, and it usually presents with multiple cranial neurophaties. It has been associated with a variety of inflammatory, infectious, traumatic, toxic and neoplasic diseases, when no specific cause is found the process is called idiopathic. The infectious cases occur in patients under systemic immunosuppression, which have an evident contiguous source or those who have undergone neurosurgical procedures. We describe a case of a 62-year-old immunosuppressed woman with diabetes and rheumatoid arthritis, which had HCP and osteomyelitis of the skull base caused by pseudomonas aeruginosa, presenting with headache and diplopia. We believe this is the second documented case of pachymeningitis secondary to this microorganism. As a multifactorial disease, it is essencial to determine the specific causative agent of HCP before making treatment decisions, and great care is needed with immunocompromised patients.
Keywords: Pseudomonas aeruginosa; Hypertrophic pachymeningitis; Ophtalmoplegia, optical neuropathy; Osteomyelitis; Skull base.
Figures
Similar articles
-
Pachymeningitis with multiple cranial neuropathies and unilateral optic neuropathy secondary to Pseudomonas aeruginosa: case report and review.J Neuroophthalmol. 1998 Sep;18(3):196-200. J Neuroophthalmol. 1998. PMID: 9736205
-
Hypertrophic cranial pachymeningitis and orbital apex syndrome secondary to infection of the eye: illustrative case.J Neurosurg Case Lessons. 2021 May 24;1(21):CASE20168. doi: 10.3171/CASE20168. eCollection 2021 May 24. J Neurosurg Case Lessons. 2021. PMID: 35854865 Free PMC article.
-
Extensive anterior cranial fossa idiopathic hypertrophic pachymeningitis: a case report and review of the literature.J Med Assoc Thai. 2005 Dec;88(12):1934-40. J Med Assoc Thai. 2005. PMID: 16518996 Review.
-
[Hypertrophic cranial pachymeningitis as a rare cause of headache].Nervenarzt. 2006 Apr;77(4):423-9. doi: 10.1007/s00115-005-2012-8. Nervenarzt. 2006. PMID: 16283149 Review. German.
-
Idiopathic hypertrophic pachymeningitis.Neurology. 2004 Mar 9;62(5):686-94. doi: 10.1212/01.wnl.0000113748.53023.b7. Neurology. 2004. PMID: 15007115 Review.
Cited by
-
The protective effects of antigen-specific IgY on pyocyanin-treated human lymphoma Raji cells.F1000Res. 2019 Jul 4;8:1008. doi: 10.12688/f1000research.19327.2. eCollection 2019. F1000Res. 2019. PMID: 32025288 Free PMC article.
References
-
- Riku S, Kato S. Idiopathic hypertrophic pachymeningitis. Neuropathology. 2003;23(4):335–344. - PubMed
-
- Mamelak AN, Kelly WM, Davis RL, Rosenblum ML. Idiopathic hypertrophic cranial pachymeningitis. Report of three cases. J Neurosurg. 1993;79(2):270–276. - PubMed
-
- Fujimoto M, Kira J, Murai H, Yoshimura T, Takizawa K, Goto I. Hypertrophic cranial pachymeningitis associated with mixed connective tissue disease; a comparison with idiopathic and infectious pachymeningitis. Intern Med. 1993;32(6):510–512. - PubMed
-
- Pareja-Esteban J, Gutierrez-Solana S, Cedazo M, Sanchez-Cordon B, Gamo-Gallego M, Teus MA. Hypertrophic pachymeningitis and ophthalmological disturbances: description of two case reports. Arch Soc Esp Oftalmol. 2008;83(8):497–500. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous