

Effect of iron therapy on platelet counts in patients with inflammatory bowel disease-associated anemia
- PMID: 22506024
- PMCID: PMC3323537
- DOI: 10.1371/journal.pone.0034520
Effect of iron therapy on platelet counts in patients with inflammatory bowel disease-associated anemia
Abstract
Background and aims: Secondary thrombocytosis is a clinical feature of unknown significance. In inflammatory bowel disease (IBD), thrombocytosis is considered a marker of active disease; however, iron deficiency itself may trigger platelet generation. In this study we tested the effect of iron therapy on platelet counts in patients with IBD-associated anemia.
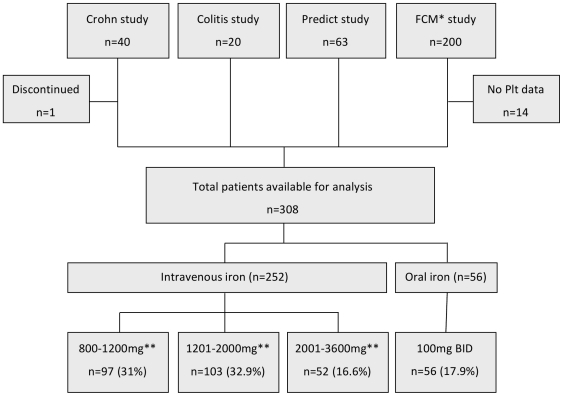
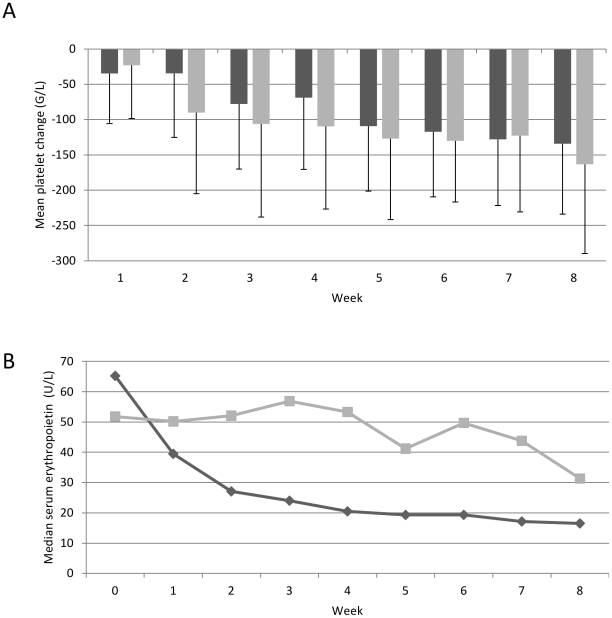
Methods: Platelet counts were analyzed before and after iron therapy from four prospective clinical trials. Further, changes in hemoglobin, transferrin saturation, ferritin, C-reactive protein, and leukocyte counts, before and after iron therapy were compared. In a subgroup the effect of erythropoietin treatment was tested. The results were confirmed in a large independent cohort (FERGIcor).
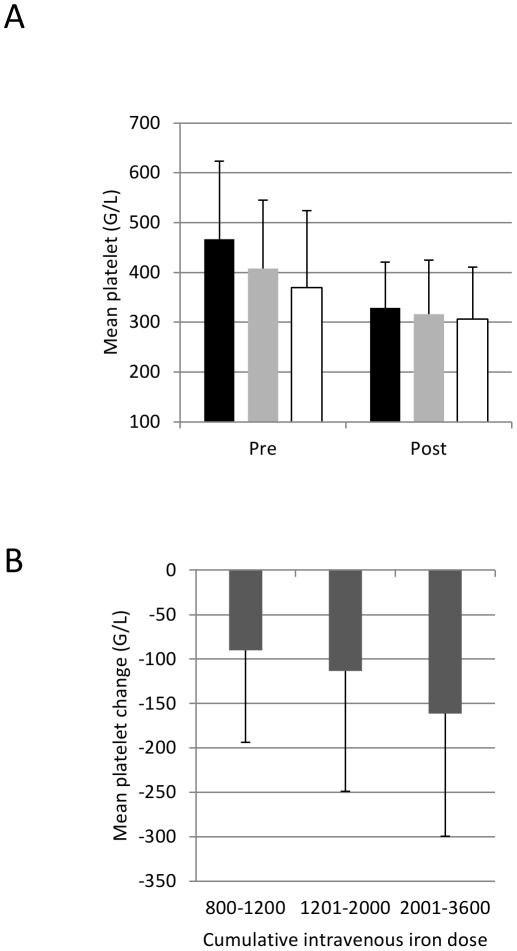
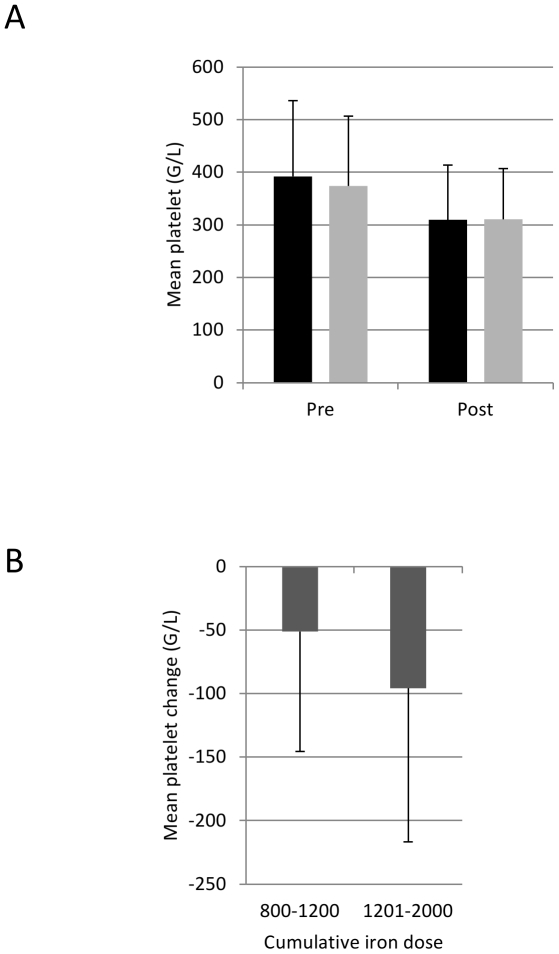
Results: A total of 308 patient records were available for the initial analysis. A dose-depended drop in platelet counts (mean 425 G/L to 320 G/L; p<0.001) was found regardless of the type of iron preparation (iron sulphate, iron sucrose, or ferric carboxymaltose). Concomitant erythropoietin therapy as well as parameters of inflammation (leukocyte counts, C-reactive protein) had no effect on the change in platelet counts. This effect of iron therapy on platelets was confirmed in the FERGIcor study cohort (n=448, mean platelet counts before iron therapy: 383 G/L, after: 310 G/L, p<0.001).
Conclusion: Iron therapy normalizes elevated platelet counts in patients with IBD-associated anemia. Thus, iron deficiency is an important pathogenetic mechanism of secondary thrombocytosis in IBD.
Conflict of interest statement
Figures
References
-
- Linden MD, Jackson DE. Platelets: Pleiotropic roles in atherogenesis and atherothrombosis. Int J Biochem Cell Biol 2010 - PubMed
-
- McMorran BJ, Marshall VM, de Graaf GC, Drysdale KE, Shabbar M, et al. Platelets kill intraerythrocytic malarial parasites and mediate survival to infection. Science. 2009;323:797–800. - PubMed
-
- Schafer AI. Thrombocytosis and thrombocythemia. Blood Rev. 2001;15:159–166. - PubMed
-
- Ceresa IF, Noris P, Ambaglio C, Pecci A, Balduini CL. Thrombopoietin is not uniquely responsible for thrombocytosis in inflammatory disorders. Platelets. 2007;18:579–582. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
