

Ovarian Cancer Is an Imported Disease: Fact or Fiction?
- PMID: 22506137
- PMCID: PMC3322388
- DOI: 10.1007/s13669-011-0004-1
Ovarian Cancer Is an Imported Disease: Fact or Fiction?
Abstract
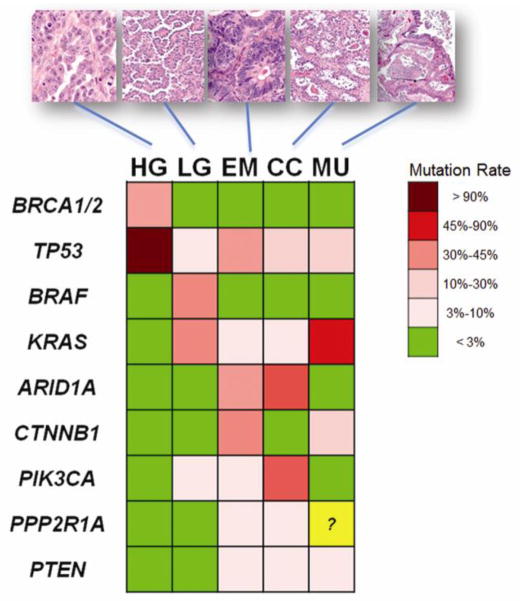
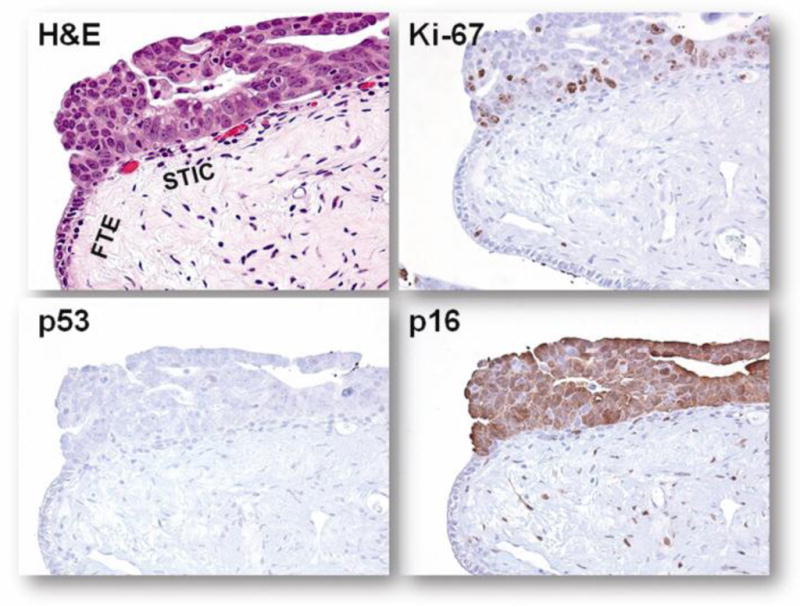
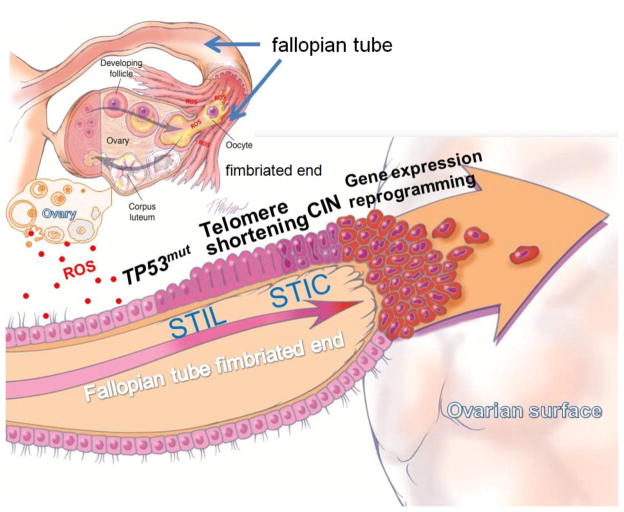
The cell of origin of ovarian cancer has been long debated. The current paradigm is that epithelial ovarian cancer (EOC) arises from the ovarian surface epithelium (OSE). OSE is composed of flat, nondescript cells more closely resembling the mesothelium lining the peritoneal cavity, with which it is continuous, rather than the various histologic types of ovarian carcinoma (serous, endometrioid, and clear cell carcinoma), which have a Müllerian phenotype. Accordingly, it has been argued that the OSE undergoes a process termed "metaplasia" to account for this profound morphologic transformation. Recent molecular and clinicopathologic studies not only have failed to support this hypothesis but also have provided evidence that EOC stems from Müllerian-derived extraovarian cells that involve the ovary secondarily, thereby calling into question the very existence of primary EOC. This new model of ovarian carcinogenesis proposes that fallopian tube epithelium (benign or malignant) implants on the ovary to give rise to both high-grade and low-grade serous carcinomas, and that endometrial tissue implants on the ovary and produces endometriosis, which can undergo malignant transformation into endometrioid and clear cell carcinoma. Thus, ultimately EOC is not ovarian in origin but rather is secondary, and it is logical to conclude that the only true primary ovarian neoplasms are germ cell and gonadal stromal tumors analogous to tumors in the testis. If this new model is confirmed, it has profound implications for the early detection and treatment of "ovarian cancer."
Conflict of interest statement
No potential conflicts of interest relevant to this article were reported.
Figures
References
-
- Buys SS, Partridge E, Black A, et al. Effect of screening on ovarian cancer mortality: the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Randomized Controlled Trial. JAMA. 2011;305:2295–2303. This population-based study analyzed the PLCO cases in an attempt to determine whether CA125 and an imaging study can save the lives of ovarian cancer patients. The study result provides cogent evidence of a lack of effective screening to reduce ovarian cancer deaths. - PubMed
-
- Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Fishman DA, Cohen L, Blank SV, et al. The role of ultrasound evaluation in the detection of early-stage epithelial ovarian cancer. Am J Obstet Gynecol. 2005;192:1214–1221. discussion 1221–1212. - PubMed
-
- Seidman JD, Cho K, Ronnett BM, et al. Surface epithelial tumors of the ovary. In: Kurman RJ, Ellenson LH, Ronnett BM, editors. Blaustein’s Pathology of the Female Genital Tract. New York: Springer Verlag; 2011. pp. 679–784.