

Renal tubular dysfunction during long-term adefovir or tenofovir therapy in chronic hepatitis B
- PMID: 22506503
- PMCID: PMC3443969
- DOI: 10.1111/j.1365-2036.2012.05093.x
Renal tubular dysfunction during long-term adefovir or tenofovir therapy in chronic hepatitis B
Abstract
Background: Adefovir and tenofovir are nucleotide analogues used as long-term therapy of chronic hepatitis B. Side effects are few, but prolonged and high-dose therapy has been associated with proximal renal tubular dysfunction (RTD).
Aim: To assess the incidence of RTD during long-term nucleotide therapy of chronic hepatitis B.
Methods: A total of 51 patients being treated at the Clinical Center, National Institutes of Health were studied. Diagnosis of RTD required de novo appearance of at least three of five features: hypophosphataemia, hypouricaemia, serum creatinine elevation, proteinuria or glucosuria.
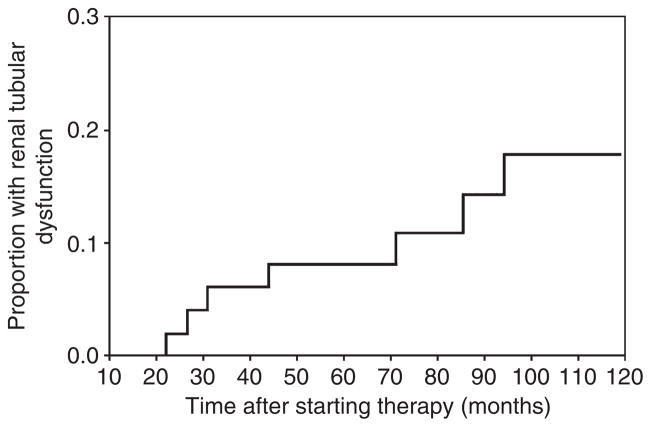
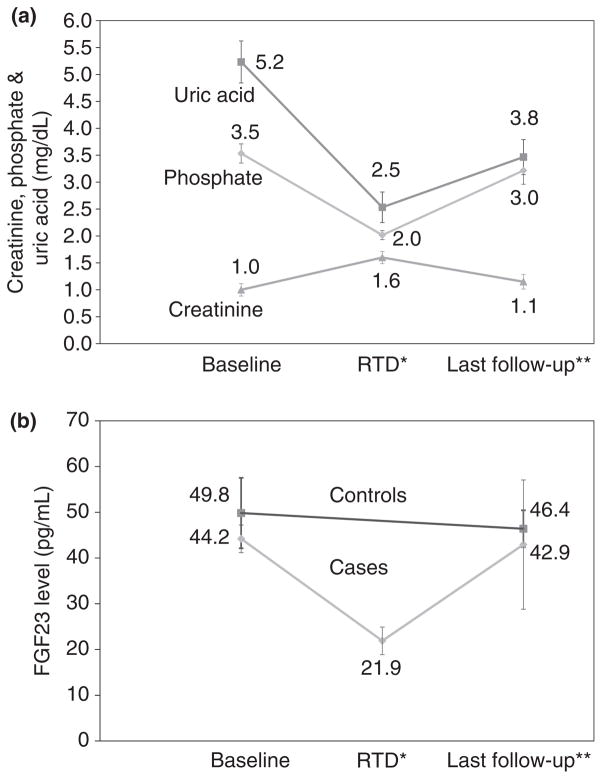
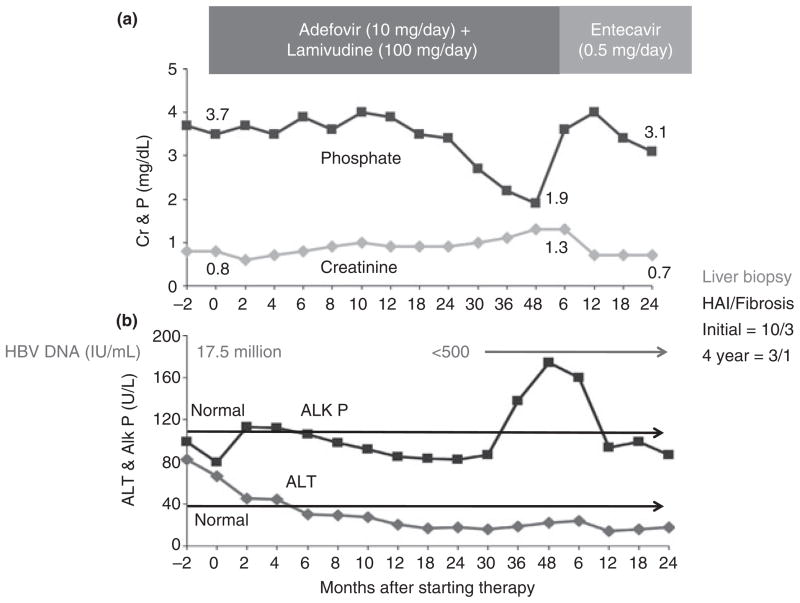
Results: Among 51 patients treated for 1-10 (mean 7.4) years with adefovir (n = 42), tenofovir (n = 4) or adefovir followed by tenofovir (n = 5), 7 (14%) developed RTD. Time to onset ranged from 22 to 94 (mean 49) months with an estimated 10-year cumulative rate of 15%. All seven had low urinary percent maximal tubular reabsorption of phosphate (<82%). Patients with RTD were older (58 vs. 44 years; P = 0.01) and had lower baseline glomerular filtration rates (82 vs. 97 cc/min; P = 0.08) compared to those without; but did not differ in other features. Six patients with RTD were switched to entecavir, all subsequently had improvements in serum phosphate (2.0-3.0 mg/dL), creatinine (1.6-1.1 mg/dL), uric acid (2.7-3.8 mg/dL) and proteinuria.
Conclusions: Renal tubular dysfunction develops in 15% of patients treated with adefovir or tenofovir for 2-9 years and is partially reversible with change to other antivirals. Monitoring for serum phosphate, creatinine and urinalysis is prudent during long-term adefovir and tenofovir therapy.
Published 2012. This article is a US Government work and is in the public domain in the USA.
Conflict of interest statement
Figures
Comment in
-
Letter: renal tubular dysfunction during nucleotide analogue therapy in chronic hepatitis B.Aliment Pharmacol Ther. 2012 Nov;36(10):992-3; author reply 993. doi: 10.1111/apt.12065. Aliment Pharmacol Ther. 2012. PMID: 23072605 No abstract available.
References
-
- Ganem D, Prince AM. Hepatitis B virus infection - natural history and clinical consequences. N Engl J Med. 2004;350:1118–29. - PubMed
-
- Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health consensus development conference statement: management of hepatitis B. Hepatology. 2009;49:S4–12. - PubMed
-
- Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology. 2009;50:661–2. - PubMed
-
- Dienstag JL, Schiff ER, Wright TL, et al. Lamivudine as initial treatment for chronic hepatitis B in the United States. N Engl J Med. 1999;341:1256–63. - PubMed
-
- Lai CL, Chien RN, Leung NW, et al. A one-year trial of lamivudine for chronic hepatitis B. Asia Hepatitis Lamivudine Study Group. N Engl J Med. 1998;339:61–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical