

A randomized comparative effectiveness study of oral triple therapy versus etanercept plus methotrexate in early aggressive rheumatoid arthritis: the treatment of Early Aggressive Rheumatoid Arthritis Trial
- PMID: 22508468
- PMCID: PMC4036119
- DOI: 10.1002/art.34498
A randomized comparative effectiveness study of oral triple therapy versus etanercept plus methotrexate in early aggressive rheumatoid arthritis: the treatment of Early Aggressive Rheumatoid Arthritis Trial
Abstract
Objective: To assess whether it is better to intensively treat all patients with early rheumatoid arthritis (RA) using combinations of drugs or to reserve this approach for patients who do not have an appropriate response (as determined by a Disease Activity Score in 28 joints using the erythrocyte sedimentation rate [DAS28-ESR] of ≥ 3.2 at week 24) to methotrexate (MTX) monotherapy, and to assess whether combination therapy with MTX plus etanercept is superior to the combination of MTX plus sulfasalazine plus hydroxychloroquine.
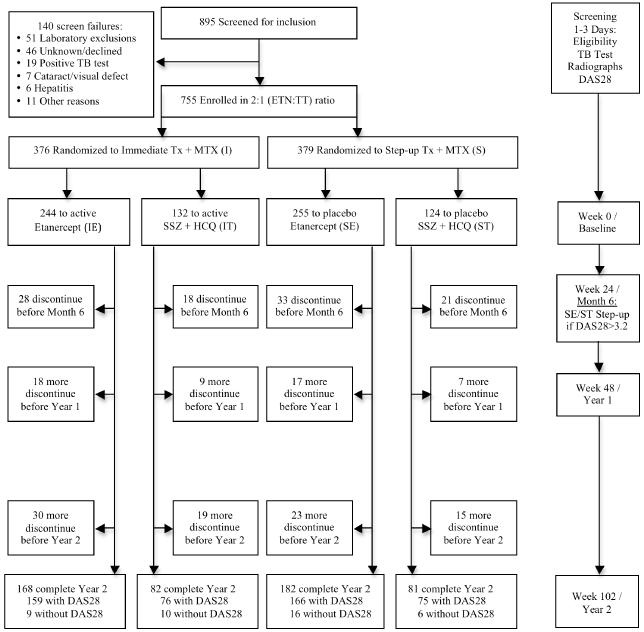
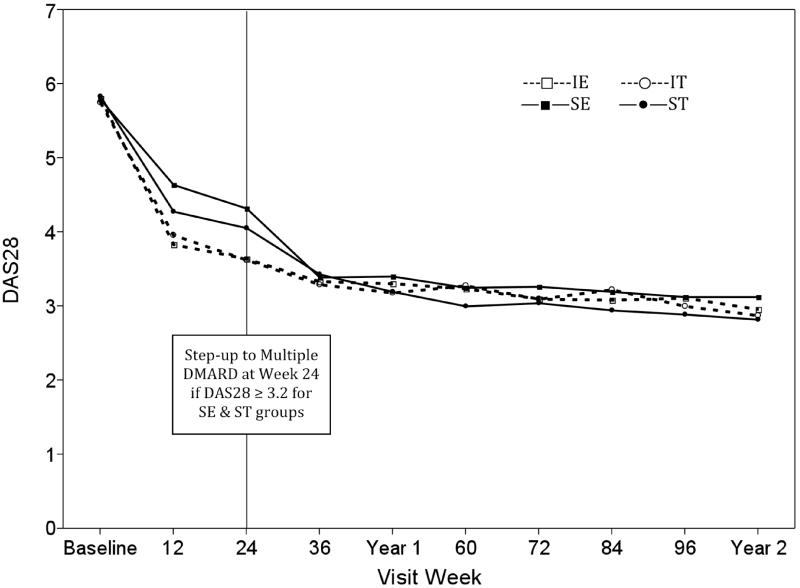
Methods: The Treatment of Early Aggressive Rheumatoid Arthritis (TEAR) study is a 2-year, randomized, double-blind trial. A 2 × 2 factorial design was used to randomly assign subjects to 1 of 4 treatment arms: immediate treatment with MTX plus etanercept, immediate oral triple therapy (MTX plus sulfasalazine plus hydroxychloroquine), or step-up from MTX monotherapy to one of the combination therapies (MTX plus etanercept or MTX plus sulfasalazine plus hydroxychloroquine) at week 24 if the DAS28-ESR was ≥ 3.2. All treatment arms included matching placebos. The primary outcome was an observed-group analysis of DAS28-ESR values from week 48 to week 102.
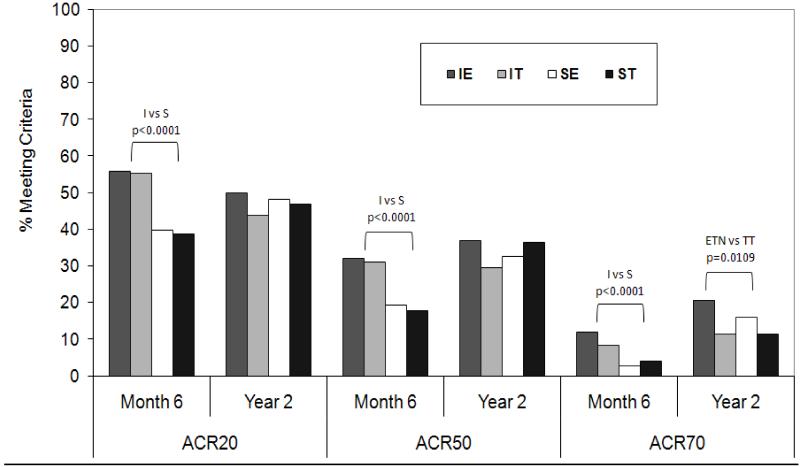
Results: At week 24 (beginning of the step-up period), subjects in the 2 immediate-treatment groups demonstrated a greater reduction in the DAS28-ESR compared with those in the 2 step-up groups (3.6 versus 4.2; P < 0.0001); no differences between the combination-therapy regimens were observed. Between week 48 and week 102, subjects randomized to the step-up arms had a DAS28-ESR clinical response that was not different from that of subjects who initially received combination therapy, regardless of the treatment arm. There was no significant difference in the DAS28-ESR between subjects randomized to oral triple therapy and those randomized to receive MTX plus etanercept. By week 102, there was a statistically significant difference in the change in radiographic measurements from baseline between the group receiving MTX plus etanercept and the group receiving oral triple therapy (0.64 versus 1.69; P = 0.047).
Conclusion: There were no differences in the mean DAS28-ESR during weeks 48-102 between subjects randomized to receive MTX plus etanercept and those randomized to triple therapy, regardless of whether they received immediate combination treatment or step-up from MTX monotherapy. At 102 weeks, immediate combination treatment with either strategy was more effective than MTX monotherapy prior to the initiation of step-up therapy. Initial use of MTX monotherapy with the addition of sulfasalazine plus hydroxychloroquine (or etanercept, if necessary, after 6 months) is a reasonable therapeutic strategy for patients with early RA. Treatment with the combination of MTX plus etanercept resulted in a statistically significant radiographic benefit compared with oral triple therapy.
Trial registration: ClinicalTrials.gov NCT00259610.
Copyright © 2012 by the American College of Rheumatology.
Figures
Comment in
-
Reply: The effect of triple therapy versus etanercept plus methotrexate in rheumatoid arthritis: comment on the article by Moreland et al.Arthritis Rheum. 2013 Feb;65(2):539-40. doi: 10.1002/art.37756. Arthritis Rheum. 2013. PMID: 23124989 No abstract available.
-
The effect of triple therapy versus etanercept plus methotrexate in rheumatoid arthritis: comment on the article by Moreland et al.Arthritis Rheum. 2013 Feb;65(2):539. doi: 10.1002/art.37757. Arthritis Rheum. 2013. PMID: 23125025 No abstract available.
References
-
- Moreland LW, Baumgartner SW, Schiff MH, Tindall EA, Fleischmann RM, Weaver AL, et al. Treatment of rheumatoid arthritis with a recombinant human tumor necrosis factor receptor (p75)-Fc fusion protein. N Engl J Med. 1997;337(3):141–7. - PubMed
-
- Lipsky PE, van der Heijde DM, St Clair EW, Furst DE, Breedveld FC, Kalden JR, et al. Infliximab and methotrexate in the treatment of rheumatoid arthritis. Anti-Tumor Necrosis Factor Trial in Rheumatoid Arthritis with Concomitant Therapy Study Group. N Engl J Med. 2000;343(22):1594–602. - PubMed
-
- Breedveld FC, Weisman MH, Kavanaugh AF, Cohen SB, Pavelka K, van Vollenhoven R, et al. The PREMIER study: A multicenter, randomized, double-blind clinical trial of combination therapy with adalimumab plus methotrexate versus methotrexate alone or adalimumab alone in patients with early, aggressive rheumatoid arthritis who had not had previous methotrexate treatment. Arthritis Rheum. 2006;54(1):26–37. - PubMed
-
- Emery P, Breedveld FC, Hall S, Durez P, Chang DJ, Robertson D, et al. Comparison of methotrexate monotherapy with a combination of methotrexate and etanercept in active, early, moderate to severe rheumatoid arthritis (COMET): a randomised, double-blind, parallel treatment trial. Lancet. 2008;372(9636):375–82. - PubMed
-
- Smolen JS, Van Der Heijde DM, St Clair EW, Emery P, Bathon JM, Keystone E, et al. Predictors of joint damage in patients with early rheumatoid arthritis treated with high-dose methotrexate with or without concomitant infliximab: results from the ASPIRE trial. Arthritis Rheum. 2006;54(3):702–10. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
