

Prospective, observational study of pain and analgesic prescribing in medical oncology outpatients with breast, colorectal, lung, or prostate cancer
- PMID: 22508819
- PMCID: PMC3383175
- DOI: 10.1200/JCO.2011.39.2381
Prospective, observational study of pain and analgesic prescribing in medical oncology outpatients with breast, colorectal, lung, or prostate cancer
Abstract
Purpose: Pain is prevalent among patients with cancer, yet pain management patterns in outpatient oncology are poorly understood.
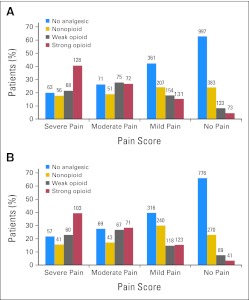
Patients and methods: A total of 3,123 ambulatory patients with invasive cancer of the breast, prostate, colon/rectum, or lung were enrolled onto this prospective study regardless of phase of care or stage of disease. At initial assessment and 4 to 5 weeks later, patients completed a 25-item measure of pain, functional interference, and other symptoms. Providers recorded analgesic prescribing. The pain management index was calculated to assess treatment adequacy.
Results: Of the 3,023 patients we identified to be at risk for pain, 2,026 (67%) reported having pain or requiring analgesics at initial assessment; of these 2,026 patients, 670 (33%) were receiving inadequate analgesic prescribing. We found no difference in treatment adequacy between the initial and follow-up visits. Multivariable analysis revealed that the odds of a non-Hispanic white patient having inadequate pain treatment were approximately half those of a minority patient after adjusting for other explanatory variables (odds ratio, 0.51; 95% CI, 0.37 to 0.70; P = .002). Other significant predictors of inadequate pain treatment were having a good performance status, being treated at a minority treatment site, and having nonadvanced disease without concurrent treatment.
Conclusion: Most outpatients with common solid tumors must confront issues related to pain and the use of analgesics. There is significant disparity in pain treatment adequacy, with the odds of undertreatment twice as high for minority patients. These findings persist over 1 month of follow-up, highlighting the complexity of these problems.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures

Comment in
-
Why is management of cancer pain still a problem?J Clin Oncol. 2012 Jun 1;30(16):1907-8. doi: 10.1200/JCO.2011.41.3146. Epub 2012 Apr 16. J Clin Oncol. 2012. PMID: 22508809 No abstract available.
-
Palliative care: Analgesia prescribing in the USA--no gain, much pain.Nat Rev Clin Oncol. 2012 May 1;9(6):306. doi: 10.1038/nrclinonc.2012.81. Nat Rev Clin Oncol. 2012. PMID: 22547219 No abstract available.
-
Clinically based palliative care training is needed urgently for all oncologists.J Clin Oncol. 2012 Nov 10;30(32):4042-3; author reply 4043-4. doi: 10.1200/JCO.2012.45.3548. Epub 2012 Sep 17. J Clin Oncol. 2012. PMID: 22987079 No abstract available.
References
-
- van den Beuken-van Everdingen MH, de Rijke JM, Kessels AG, et al. Prevalence of pain in patients with cancer: A systematic review of the past 40 years. Ann Oncol. 2007;18:1437–1449. - PubMed
-
- Cleeland CS, Gonin R, Hatfield AK, et al. Pain and its treatment in outpatients with metastatic cancer. N Engl J Med. 1994;330:592–596. - PubMed
-
- Patrick DL, Ferketich SL, Frame PS, et al. National Institutes of Health State-of-the-Science Conference Statement: Symptom management in cancer—Pain, depression, and fatigue, July 15-17, 2002. J Natl Cancer Inst Monogr. 2004:9–16. - PubMed
-
- Eastern Cooperative Oncology Group: SOAPP (Symptom Outcomes and Practice Patterns): A Survey of Disease and Treatment-Related Symptoms in Patients With Invasive Cancer of the Breast, Prostate, Lung, or Colon/Rectum. http://www.ecogsoapp.com.
-
- Cleeland CS, Mendoza TR, Wang XS, et al. Assessing symptom distress in cancer patients: The M.D. Anderson Symptom Inventory. Cancer. 2000;89:1634–1646. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
