

Left ventricular failure produces profound lung remodeling and pulmonary hypertension in mice: heart failure causes severe lung disease
- PMID: 22508832
- PMCID: PMC3402091
- DOI: 10.1161/HYPERTENSIONAHA.111.186072
Left ventricular failure produces profound lung remodeling and pulmonary hypertension in mice: heart failure causes severe lung disease
Abstract
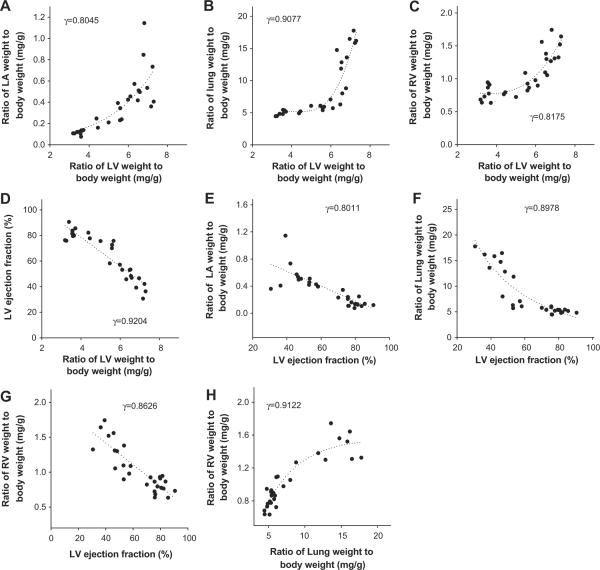
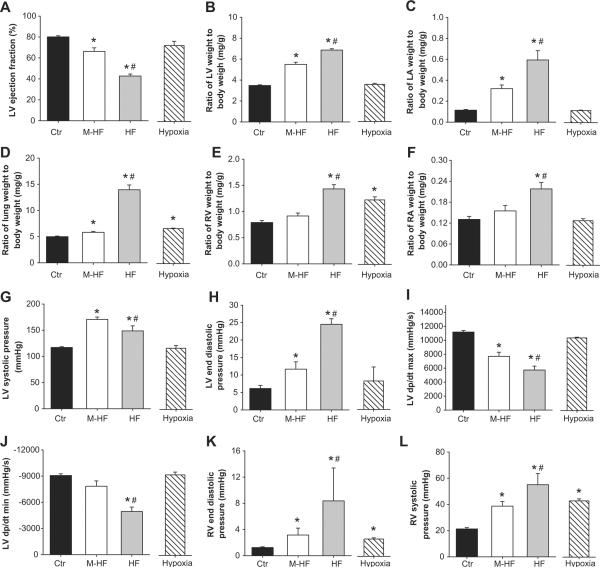
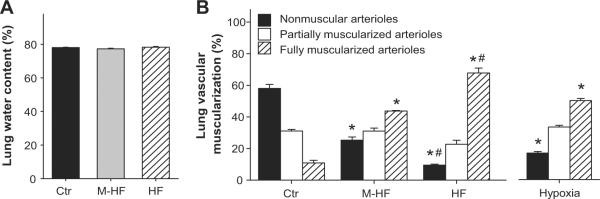
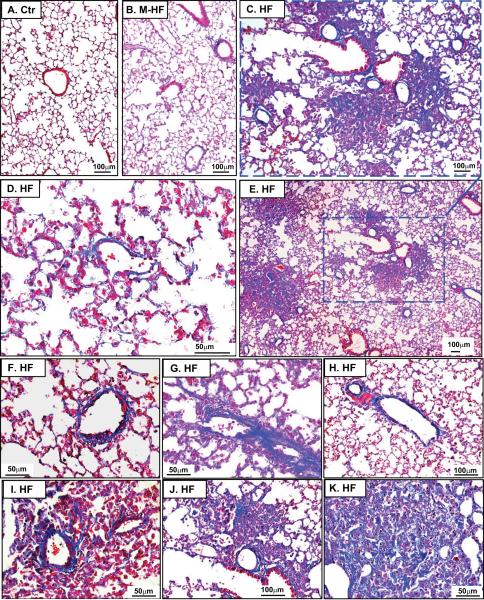
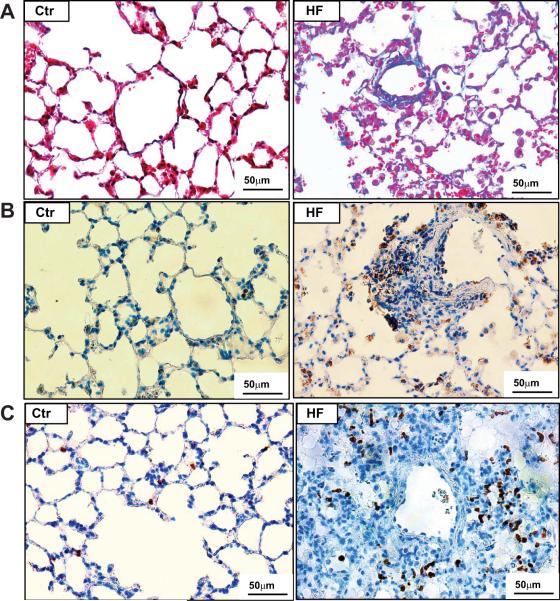
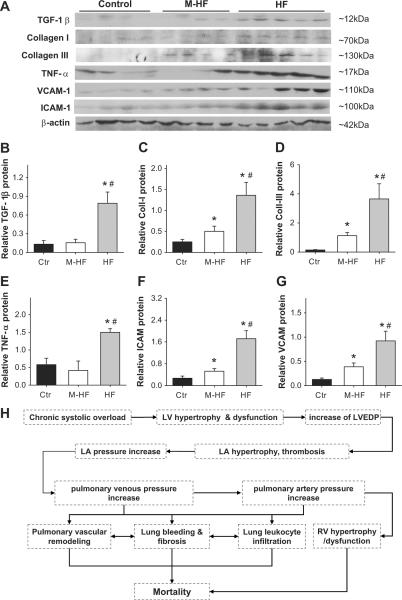
Chronic left ventricular failure causes pulmonary congestion with increased lung weight and type 2 pulmonary hypertension. Understanding the molecular mechanisms for type 2 pulmonary hypertension and the development of novel treatments for this condition requires a robust experimental animal model and a good understanding of the nature of the resultant pulmonary remodeling. Here we demonstrate that chronic transverse aortic constriction causes massive pulmonary fibrosis and remodeling, as well as type 2 pulmonary hypertension, in mice. Thus, aortic constriction-induced left ventricular dysfunction and increased left ventricular end-diastolic pressure are associated with a ≤5.3-fold increase in lung wet weight and dry weight, pulmonary hypertension, and right ventricular hypertrophy. Interestingly, the aortic constriction-induced increase in lung weight was not associated with pulmonary edema but resulted from profound pulmonary remodeling with a dramatic increase in the percentage of fully muscularized lung vessels, marked vascular and lung fibrosis, myofibroblast proliferation, and leukocyte infiltration. The aortic constriction-induced left ventricular dysfunction was also associated with right ventricular hypertrophy, increased right ventricular end-diastolic pressure, and right atrial hypertrophy. The massive lung fibrosis, leukocyte infiltration, and pulmonary hypertension in mice after transverse aortic constriction clearly indicate that congestive heart failure also causes severe lung disease. The lung fibrosis and leukocyte infiltration may be important mechanisms in the poor clinical outcome in patients with end-stage heart failure. Thus, the effective treatment of left ventricular failure may require additional efforts to reduce lung fibrosis and the inflammatory response.
Figures
References
-
- Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, Denton CP, Elliott CG, Gaine SP, Gladwin MT, Jing ZC, Krowka MJ, Langleben D, Nakanishi N, Souza R. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009;54(1 Suppl):S43–54. - PubMed
-
- Cournand A, Bloomfield RA, Lauson HD. Double lumen catheter for intravenous and intracardiac blood sampling and pressure recording. Proc Soc Exp Biol Med. 1945;60:73–75. - PubMed
-
- Galié N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, Beghetti M, Corris P, Gaine S, Gibbs JS, Gomez-Sanchez MA, Jondeau G, Klepetko W, Opitz C, Peacock A, Rubin L, Zellweger M, Simonneau G. Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2009;34:1219–1263. - PubMed
-
- Hoeper MM, Barberá JA, Channick RN, Hassoun PM, Lang IM, Manes A, Martinez FJ, Naeije R, Olschewski H, Pepke-Zaba J, Redfield MM, Robbins IM, Souza R, Torbicki A, McGoon M. Diagnosis, assessment, and treatment of non-pulmonary arterial hypertension pulmonary hypertension. J Am Coll Cardiol. 2009;54(1 Suppl):S85–96. - PubMed
-
- Grigioni F, Potena L, Galié N, Fallani F, Bigliardi M, Coccolo F, Magnani G, Manes A, Barbieri A, Fucili A, Magelli C, Branzi A. Prognostic implications of serial assessments of pulmonary hypertension in severe chronic heart failure. J Heart Lung Transplant. 2006;25:1241–1246. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
