

Barriers to medication adherence in HIV-infected children and youth based on self- and caregiver report
- PMID: 22508915
- PMCID: PMC3340587
- DOI: 10.1542/peds.2011-1740
Barriers to medication adherence in HIV-infected children and youth based on self- and caregiver report
Abstract
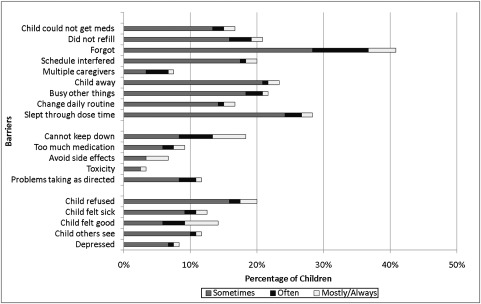
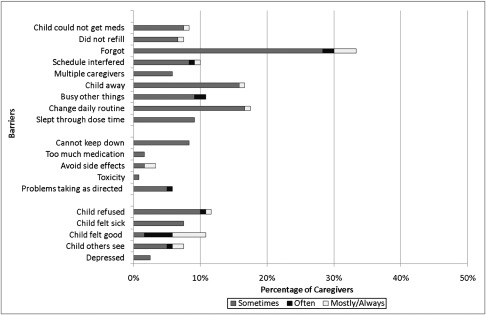
Objective: Nonadherence to antiretroviral therapy among children/youth with HIV often is associated with disease progression. This study examined the agreement between child and caregiver perceptions of barriers to adherence and factors associated with these barriers.
Methods: Children/youth with perinatally acquired HIV and their parents/caregivers (n = 120 dyads) completed a questionnaire about 19 potential barriers to adherence to the child's antiretroviral therapy regimen. Agreement between the 2 reports was measured via the kappa statistic. Factors associated with the barriers were assessed by using multiple logistic regression.
Results: Of the 120 children, 55% were African American, 54% were boys, and the average age was 12.8 years. The most frequently reported barrier by either the caregiver or youth was "forgot." There were varying degrees of agreement between child and caregiver on the following barriers: "forgot," "taste," "child was away from home," "child refused," and "child felt good." Children who knew their HIV status were more likely to report logistical barriers, such as scheduling issues. Children with a biological parent as their caregiver were more likely to report regimen or fear of disclosure as a barrier.
Conclusions: Lack of agreement was observed for more than half of the studied barriers, indicating discrepancies between children's and caregivers' perceptions of factors that influence medication-taking. The findings suggest a need for interventions that involve both child and caregiver in the tasks of remembering when to administer the child's medications, sustaining adherence, and appropriately transitioning medication responsibility to the youth.
Figures
Comment in
-
Who forgot? The challenges of family responsibility for adherence in vulnerable pediatric populations.Pediatrics. 2012 May;129(5):e1324-5. doi: 10.1542/peds.2012-0526. Epub 2012 Apr 16. Pediatrics. 2012. PMID: 22508911 No abstract available.
References
-
- Patel K, Hernán MA, Williams PL, et al. Pediatric AIDS Clinical Trials Group 219/219C Study Team . Long-term effectiveness of highly active antiretroviral therapy on the survival of children and adolescents with HIV infection: a 10-year follow-up study. Clin Infect Dis. 2008;46(4):507–515 - PubMed
-
- Carpenter CC, Cooper DA, Fischl MA, et al. Antiretroviral therapy in adults: updated recommendations of the International AIDS Society-USA Panel. JAMA. 2000;283(3):381–390 - PubMed
-
- Brogly S, Williams P, Seage GR, III, Oleske JM, Van Dyke R, McIntosh K, PACTG 219C Team . Antiretroviral treatment in pediatric HIV infection in the United States: from clinical trials to clinical practice. JAMA. 2005;293(18):2213–2220 - PubMed
-
- Murphy DA, Sarr M, Durako SJ, Moscicki AB, Wilson CM, Muenz LR, Adolescent Medicine HIV/AIDS Research Network . Barriers to HAART adherence among human immunodeficiency virus-infected adolescents. Arch Pediatr Adolesc Med. 2003;157(3):249–255 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
