

Variability of intensive care admission decisions for the very elderly
- PMID: 22509296
- PMCID: PMC3324496
- DOI: 10.1371/journal.pone.0034387
Variability of intensive care admission decisions for the very elderly
Abstract
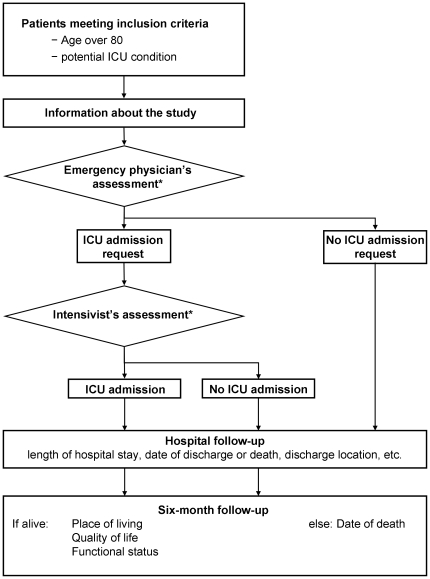
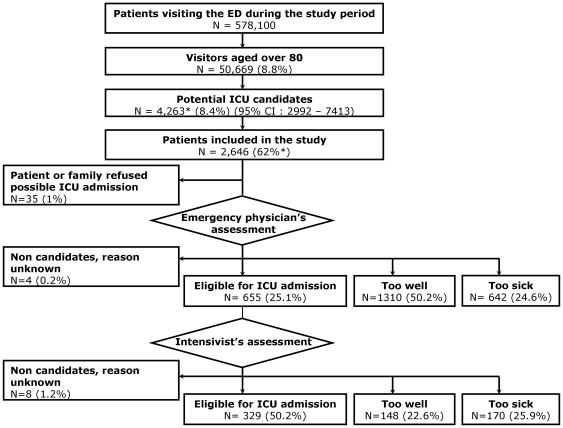
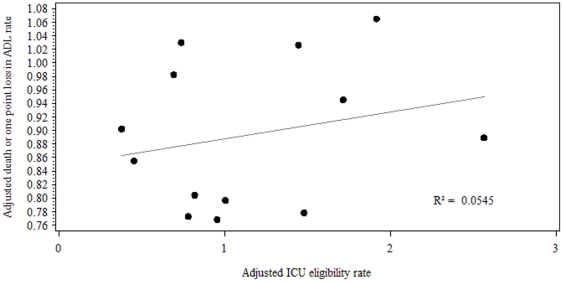
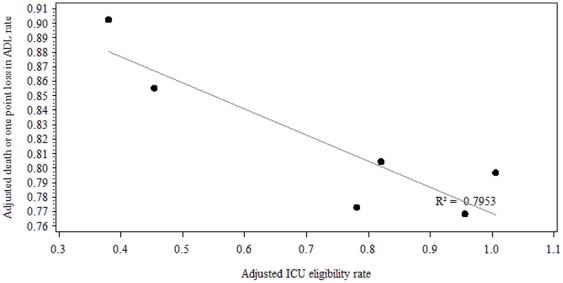
Although increasing numbers of very elderly patients are requiring intensive care, few large sample studies have investigated ICU admission of very elderly patients. Data on pre triage by physicians from other specialities is limited. This observational cohort study aims at examining inter-hospital variability of ICU admission rates and its association with patients' outcomes. All patients over 80 years possibly qualifying for ICU admission who presented to the emergency departments (ED) of 15 hospitals in the Paris (France) area during a one-year period were prospectively included in the study. Main outcome measures were ICU eligibility, as assessed by the ED and ICU physicians; in-hospital mortality; and vital and functional status 6 months after the ED visit. 2646 patients (median age 86; interquartile range 83-91) were included in the study. 94% of participants completed follow-up (n = 2495). 12.4% (n = 329) of participants were deemed eligible for ICU admission by ED physicians and intensivists. The overall in-hospital and 6-month mortality rates were respectively 27.2% (n = 717) and 50.7% (n = 1264). At six months, 57.5% (n = 1433) of patients had died or had a functional deterioration. Rates of patients deemed eligible for ICU admission ranged from 5.6% to 38.8% across the participating centers, and this variability persisted after adjustment for patients' characteristics. Despite this variability, we found no association between level of ICU eligibility and either in-hospital death or six-month death or functional deterioration. In France, the likelihood that a very elderly person will be admitted to an ICU varies widely from one hospital to another. Influence of intensive care admission on patients' outcome remains unclear.
Trial registration: ClinicalTrials.gov NCT00912600.
Conflict of interest statement
Figures
References
-
- Wilson DM, Thurston A, Lichlyter B. Should the oldest-old be admitted to the intensive care unit and receive advanced life-supporting care? Crit Care Med. 2010;38:303–304. doi: 10.1097/CCM.0b013e3181b4a263. - DOI - PubMed
-
- Nguyen Y-L, Angus DC, Boumendil A, Guidet B. The challenge of admitting the very elderly to intensive care. Ann Intensive Care. 2011;1:29. doi: 10.1186/2110-5820-1-29. - DOI - PMC - PubMed
-
- Azoulay E, Pochard F, Chevret S, Vinsonneau C, Garrouste M, et al. Compliance with triage to intensive care recommendations. Crit Care Med. 2001;29:2132–2136. - PubMed
-
- Frisho-Lima P, Gurman G, Schapira A, Porath A. Rationing critical care – what happens to patients who are not admitted? Theor Surg. 1994;9:208–211. - PubMed
-
- Joynt GM, Gomersall CD, Tan P, Lee A, Cheng CA, et al. Prospective evaluation of patients refused admission to an intensive care unit: triage, futility and outcome. Intensive Care Med. 2001;27:1459–1465. doi: 10.1007/s001340101041. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
