

Low back pain subgroups using fear-avoidance model measures: results of a cluster analysis
- PMID: 22510537
- PMCID: PMC3404223
- DOI: 10.1097/AJP.0b013e31824306ed
Low back pain subgroups using fear-avoidance model measures: results of a cluster analysis
Abstract
Objectives: The purpose of this secondary analysis was to test the hypothesis that an empirically derived psychological subgrouping scheme based on multiple Fear-Avoidance Model (FAM) constructs would provide additional capabilities for clinical outcomes in comparison with a single FAM construct.
Methods: Patients (n=108) with acute or subacute low back pain enrolled in a clinical trial comparing behavioral physical therapy interventions to classification-based physical therapy completed baseline questionnaires for Pain Catastrophizing Scale, fear-avoidance beliefs [Fear-Avoidance Beliefs Questionnaire (FABQ)-physical activity scale (PA), FABQ work scale], and patient-specific fear (Fear of Daily Activities Questionnaire). Clinical outcomes included pain intensity and disability measured at baseline, 4 weeks, and 6 months. A hierarchical agglomerative cluster analysis was used to create distinct cluster profiles among the FAM measures and discriminant analysis was used to interpret clusters. Changes in clinical outcomes were investigated with repeated measures analysis of variance and differences in results based on cluster membership were compared with FABQ-PA subgrouping used in the original trial.
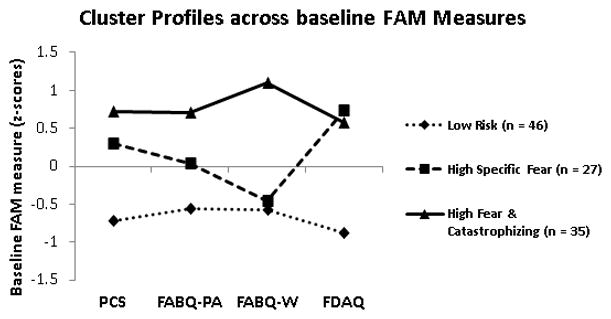
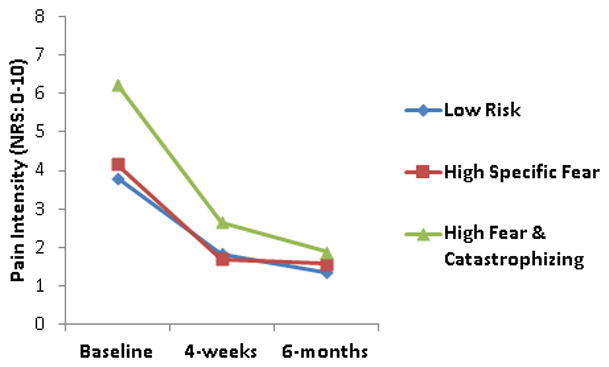
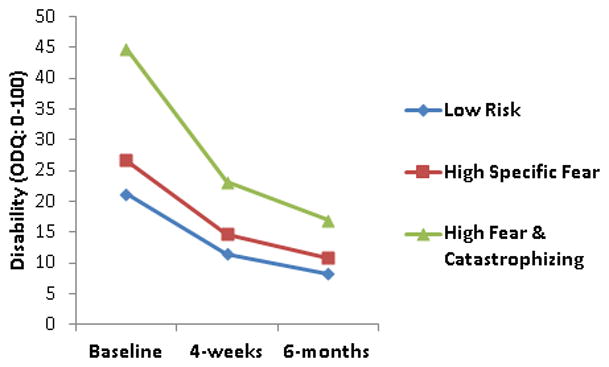
Results: Three distinct FAM subgroups (Low-Risk, High Specific Fear, and High Fear and Catastrophizing) emerged from cluster analysis. Subgroups differed on baseline pain and disability (P<0.01) with the High Fear and Catastrophizing subgroup associated with greater pain than the Low-Risk subgroup (P<0.01) and the greatest disability (P<0.05). Subgroup×time interactions were detected for both pain and disability (P<0.05) with the High Fear and Catastrophizing subgroup reporting greater changes in pain and disability than other subgroups (P<0.05). In contrast, FABQ-PA subgroups used in the original trial were not associated with interactions for clinical outcomes.
Discussion: These data suggest that subgrouping based on multiple FAM measures may provide additional information on clinical outcomes in comparison with determining subgroup status by FABQ-PA alone. Subgrouping methods for patients with low back pain should include multiple psychological factors to further explore if patients can be matched with appropriate interventions.
Figures
References
-
- Turk DC. The potential of treatment matching for subgroups of patients with chronic pain: lumping versus splitting. Clin J Pain. 2005;21(1):44–55. discussion 69–72. - PubMed
-
- Foster NE, Hill JC, Hay EM. Subgrouping patients with low back pain in primary care: are we getting any better at it? Man Ther. 2011;16(1):3–8. - PubMed
-
- Boersma K, Linton SJ. Screening to identify patients at risk: profiles of psychological risk factors for early intervention. Clin J Pain. 2005;21(1):38–43. discussion 69–72. - PubMed
-
- Vlaeyen JW, Morley S. Cognitive-behavioral treatments for chronic pain: what works for whom? Clin J Pain. 2005;21(1):1–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
