

Trends in the incidence of noncardiogenic acute respiratory failure: the role of race
- PMID: 22511134
- PMCID: PMC3329645
- DOI: 10.1097/CCM.0b013e31824518f2
Trends in the incidence of noncardiogenic acute respiratory failure: the role of race
Abstract
Objective: We sought to examine trends in the race-specific incidence of acute respiratory failure in the United States.
Design: Retrospective cohort study.
Setting: We used the National Hospital Discharge Survey database (1992-2007), an annual survey of approximately 500 hospitals weighted to provide national hospitalization estimates.
Patients: All incident cases of noncardiogenic acute respiratory failure hospitalized in the United States.
Interventions: None.
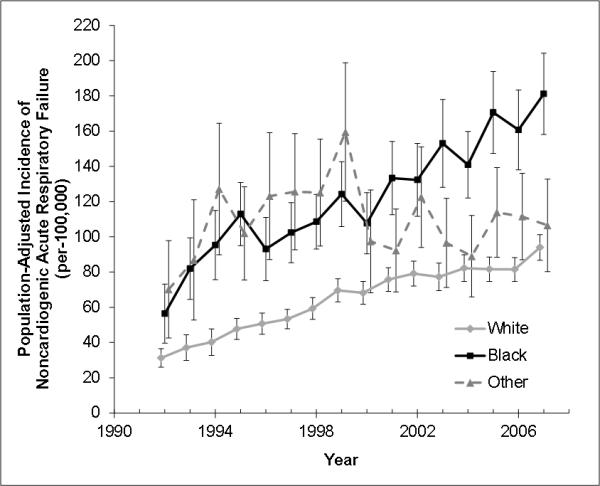
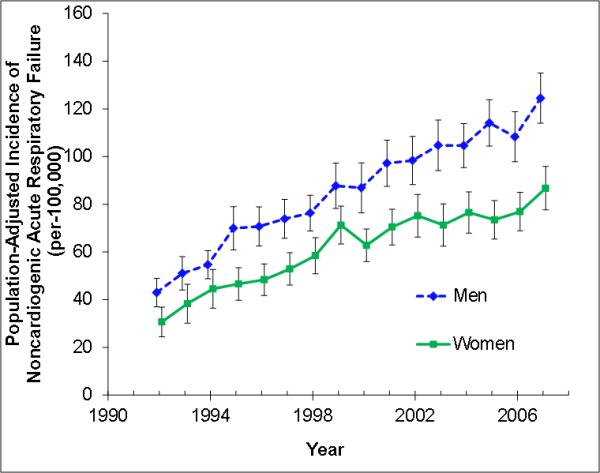
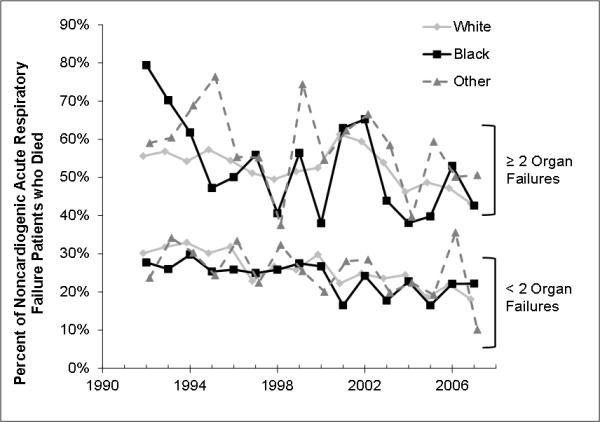
Measurements and main results: We identified noncardiogenic acute respiratory failure by the presence of International Classification of Diseases, Ninth Revision, codes for respiratory failure or pulmonary edema (518.4, 518.5, 518.81, and 518.82) and mechanical ventilation (96.7×), excluding congestive heart failure. Incidence rates were calculated using yearly census estimates standardized to the age and sex distribution of the 2000 census population. Annual cases of noncardiogenic acute respiratory failure increased from 86,755 in 1992 to 323,474 in 2007. Noncardiogenic acute respiratory failure among black Americans increased from 56.4 (95% confidence interval 39.7-73.1) to 143.8 (95% confidence interval 123.8-163.8) cases per 100,000 in 1992 and 2007, respectively. Among white Americans, the incidence of noncardiogenic acute respiratory failure increased from 31.2 (95% confidence interval 26.2-36.5) to 94.0 (95% confidence interval 86.7-101.2) cases per 100,000 in 1992 and 2007, respectively. The average annual incidence of noncardiogenic acute respiratory failure over the entire study period was 95.1 (95% confidence interval 93.9-96.4) cases per 100,000 for black Americans compared to 66.5 (95% confidence interval 65.8-67.2) cases per 100,000 for white Americans (rate ratio 1.43, 95% confidence interval 1.42-1.44). Overall in-hospital mortality was greater for other-race Americans, but only among patients with two or more organ failures (57% [95% confidence interval 56%-59%] for other race, 51% [95% confidence interval 50%-52%] for white, 50% [95% confidence interval 49%-51%] for black).
Conclusions: The incidence of noncardiogenic acute respiratory failure in the United States increased between 1992 and 2007. Black and other-race Americans are at greater risk of developing noncardiogenic acute respiratory failure compared to white Americans.
Figures
Comment in
-
Race and respiratory failure: we need to learn more.Crit Care Med. 2012 May;40(5):1674-5. doi: 10.1097/CCM.0b013e3182495937. Crit Care Med. 2012. PMID: 22511158 No abstract available.
References
-
- Smedley BD, Stith AY, Nelson AR, et al. Unequal treatment : confronting racial and ethnic disparities in health care. National Academy Press; Washington, D.C.: 2003. - PubMed
-
- Martin GS, Mannino DM, Eaton S, et al. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348(16):1546–1554. - PubMed
-
- Wunsch H, Linde-Zwirble WT, Angus DC, et al. The epidemiology of mechanical ventilation use in the United States. Crit Care Med. 2010;38(10):1947–1953. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
