

Carboplatin and paclitaxel with vs without bevacizumab in older patients with advanced non-small cell lung cancer
- PMID: 22511687
- PMCID: PMC3418968
- DOI: 10.1001/jama.2012.454
Carboplatin and paclitaxel with vs without bevacizumab in older patients with advanced non-small cell lung cancer
Abstract
Context: A previous randomized trial demonstrated that adding bevacizumab to carboplatin and paclitaxel improved survival in advanced non-small cell lung cancer (NSCLC). However, longer survival was not observed in the subgroup of patients aged 65 years or older.
Objective: To examine whether adding bevacizumab to carboplatin and paclitaxel chemotherapy is associated with improved survival in older patients with NSCLC.
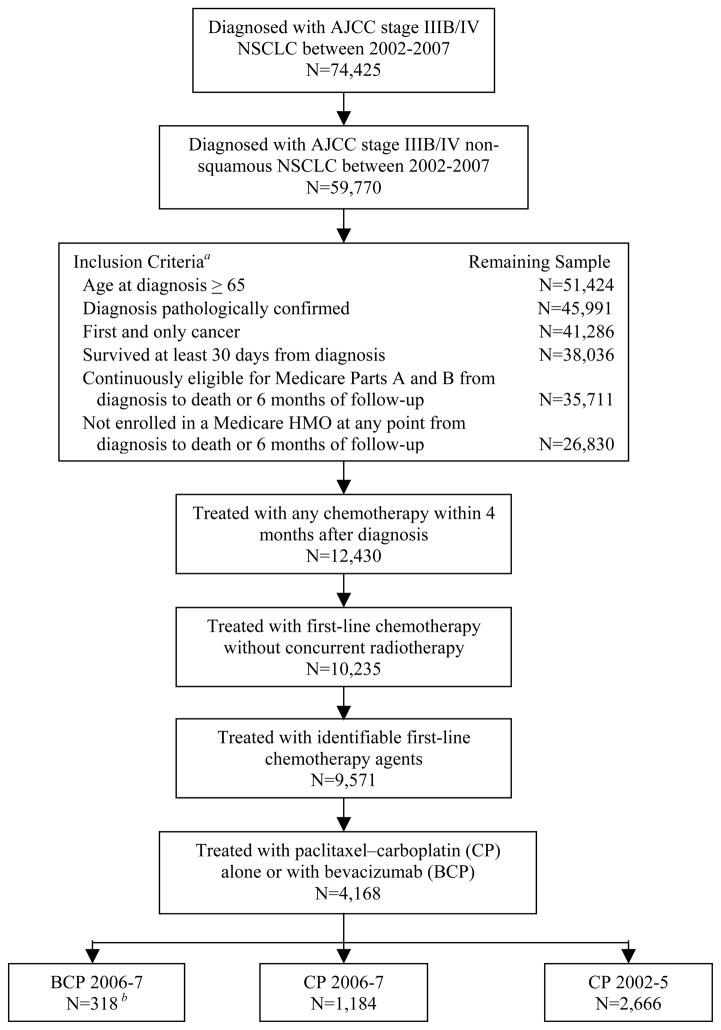
Design, setting, and participants: Retrospective cohort study of 4168 Medicare beneficiaries aged 65 years or older with stage IIIB or stage IV non-squamous cell NSCLC diagnosed in 2002-2007 in a Surveillance, Epidemiology, and End Results (SEER) region. Patients were categorized into 3 cohorts based on diagnosis year and type of initial chemotherapy administered within 4 months of diagnosis: (1) diagnosis in 2006-2007 and bevacizumab-carboplatin-paclitaxel therapy; (2) diagnosis in 2006-2007 and carboplatin-paclitaxel therapy; or (3) diagnosis in 2002-2005 and carboplatin-paclitaxel therapy. The associations between carboplatin-paclitaxel with vs without bevacizumab and overall survival were compared using Cox proportional hazards models and propensity score analyses including information about patient characteristics recorded in SEER-Medicare.
Main outcome measure: Overall survival measured from the first date of chemotherapy treatment until death or the censoring date of December 31, 2009.
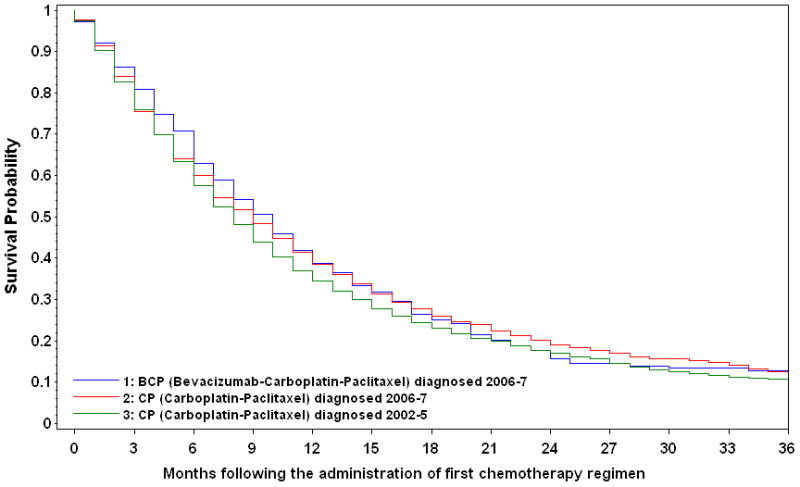
Results: The median survival estimates were 9.7 (interquartile range [IQR], 4.4-18.6) months for bevacizumab-carboplatin-paclitaxel, 8.9 (IQR, 3.5-19.3) months for carboplatin-paclitaxel in 2006-2007, and 8.0 (IQR, 3.7-17.2) months for carboplatin-paclitaxel in 2002-2005. One-year survival probabilities were 39.6% (95% CI, 34.6%-45.4%) for bevacizumab-carboplatin-paclitaxel vs 40.1% (95% CI, 37.4%-43.0%) for carboplatin-paclitaxel in 2006-2007 and 35.6% (95% CI, 33.8%-37.5%) for carboplatin-paclitaxel in 2002-2005. Neither multivariable nor propensity score-adjusted Cox models demonstrated a survival advantage for bevacizumab-carboplatin-paclitaxel compared with carboplatin-paclitaxel cohorts. In propensity score-stratified models, the hazard ratio for overall survival for bevacizumab-carboplatin-paclitaxel compared with carboplatin-paclitaxel in 2006-2007 was 1.01 (95% CI, 0.89-1.16; P = .85) and compared with carboplatin-paclitaxel in 2002-2005 was 0.93 (95% CI, 0.83-1.06; P = .28). The propensity score-weighted model and propensity score-matching model similarly failed to demonstrate a statistically significant superiority for bevacizumab-carboplatin-paclitaxel. Subgroup and sensitivity analyses for key variables did not change these findings.
Conclusion: Adding bevacizumab to carboplatin and paclitaxel chemotherapy was not associated with better survival among Medicare patients with advanced NSCLC.
Conflict of interest statement
Figures
Comment in
-
Is it time for medicine-based evidence?JAMA. 2012 Apr 18;307(15):1641-3. doi: 10.1001/jama.2012.482. JAMA. 2012. PMID: 22511693 No abstract available.
References
-
- Iannettoni MD. Staging strategies for lung cancer. JAMA. 2010;304(20):2296–2297. - PubMed
-
- Davidoff AJ, Tang M, Seal B, Edelman MJ. Chemotherapy and survival benefit in elderly patients with advanced non-small-cell lung cancer. J Clin Oncol. 2010;28(13):2191–2197. - PubMed
-
- Altekruse SF, Kosary CL, Krapcho M, et al. SEER Cancer Statistics Review. National Cancer Institute; Bethesda, MD: 1975–2007. [Accessed on August 20, 2011]. http://seer.cancer.gov/csr/1975_2007/
-
- Gridelli C, Maione P, Rossi A, De Marinis F. The role of bevacizumab in the treatment of non-small cell lung cancer: current indications and future developments. Oncologist. 2007;12(10):1183–1193. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
