

Association between helicopter vs ground emergency medical services and survival for adults with major trauma
- PMID: 22511688
- PMCID: PMC3684156
- DOI: 10.1001/jama.2012.467
Association between helicopter vs ground emergency medical services and survival for adults with major trauma
Erratum in
-
Errors in Table.JAMA. 2022 Jul 5;328(1):79. doi: 10.1001/jama.2022.8652. JAMA. 2022. PMID: 35788816 Free PMC article. No abstract available.
Abstract
Context: Helicopter emergency medical services and their possible effect on outcomes for traumatically injured patients remain a subject of debate. Because helicopter services are a limited and expensive resource, a methodologically rigorous investigation of its effectiveness compared with ground emergency medical services is warranted.
Objective: To assess the association between the use of helicopter vs ground services and survival among adults with serious traumatic injuries.
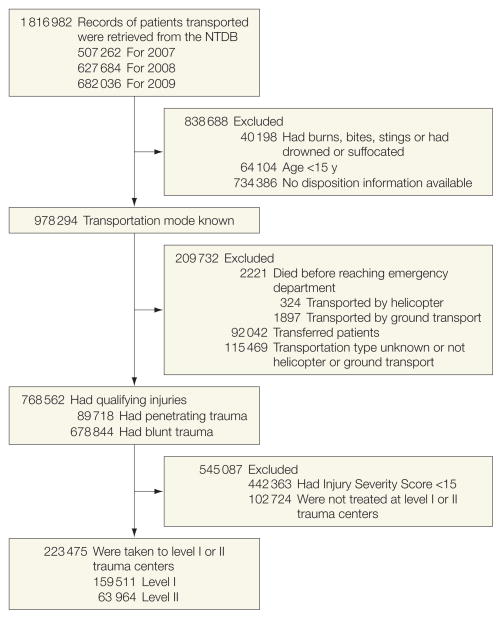
Design, setting, and participants: Retrospective cohort study involving 223,475 patients older than 15 years, having an injury severity score higher than 15, and sustaining blunt or penetrating trauma that required transport to US level I or II trauma centers and whose data were recorded in the 2007-2009 versions of the American College of Surgeons National Trauma Data Bank.
Interventions: Transport by helicopter or ground emergency services to level I or level II trauma centers.
Main outcome measures: Survival to hospital discharge and discharge disposition.
Results: A total of 61,909 patients were transported by helicopter and 161,566 patients were transported by ground. Overall, 7813 patients (12.6%) transported by helicopter died compared with 17,775 patients (11%) transported by ground services. Before propensity score matching, patients transported by helicopter to level I and level II trauma centers had higher Injury Severity Scores. In the propensity score-matched multivariable regression model, for patients transported to level I trauma centers, helicopter transport was associated with an improved odds of survival compared with ground transport (odds ratio [OR], 1.16; 95% CI, 1.14-1.17; P < .001; absolute risk reduction [ARR], 1.5%). For patients transported to level II trauma centers, helicopter transport was associated with an improved odds of survival (OR, 1.15; 95% CI, 1.13-1.17; P < .001; ARR, 1.4%). A greater proportion (18.2%) of those transported to level I trauma centers by helicopter were discharged to rehabilitation compared with 12.7% transported by ground services (P < .001), and 9.3% transported by helicopter were discharged to intermediate facilities compared with 6.5% by ground services (P < .001). Fewer patients transported by helicopter left level II trauma centers against medical advice (0.5% vs 1.0%, P < .001).
Conclusion: Among patients with major trauma admitted to level I or level II trauma centers, transport by helicopter compared with ground services was associated with improved survival to hospital discharge after controlling for multiple known confounders.
Conflict of interest statement
Figures
Comment in
-
Is it time for medicine-based evidence?JAMA. 2012 Apr 18;307(15):1641-3. doi: 10.1001/jama.2012.482. JAMA. 2012. PMID: 22511693 No abstract available.
-
Helicopter vs ground transportation for patients with trauma.JAMA. 2012 Aug 8;308(6):563; author reply 565. doi: 10.1001/jama.2012.7770. JAMA. 2012. PMID: 22871857 No abstract available.
-
Helicopter vs ground transportation for patients with trauma.JAMA. 2012 Aug 8;308(6):563-4; author reply 565. doi: 10.1001/jama.2012.7772. JAMA. 2012. PMID: 22871858 No abstract available.
-
Helicopter vs ground transportation for patients with trauma.JAMA. 2012 Aug 8;308(6):564; author reply 565. doi: 10.1001/jama.2012.7776. JAMA. 2012. PMID: 22871859 No abstract available.
-
Helicopter vs ground transportation for patients with trauma.JAMA. 2012 Aug 8;308(6):564-5; author reply 565. doi: 10.1001/jama.2012.7774. JAMA. 2012. PMID: 22871860 No abstract available.
References
-
- World Health Organization. The Global Burden of Disease: 2004 Update. Geneva, Switzerland: World Health Organization Press; 2008.
-
- Thomas SH, Cheema F, Wedel SK, Thomson D. Trauma helicopter emergency medical services transport: annotated review of selected outcomes-related literature. Prehosp Emerg Care. 2002;6(3):359–371. - PubMed
-
- Thomas SH, Biddinger PD. Helicopter trauma transport: an overview of recent outcomes and triage literature. Curr Opin Anaesthesiol. 2003;16(2):153–158. - PubMed
-
- Ringburg AN, Thomas SH, Steyerberg EW, van Lieshout EM, Patka P, Schipper IB. Lives saved by helicopter emergency medical services: an overview of literature. Air Med J. 2009;28(6):298–302. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
