

Long-term survival following partial vs radical nephrectomy among older patients with early-stage kidney cancer
- PMID: 22511691
- PMCID: PMC3864575
- DOI: 10.1001/jama.2012.475
Long-term survival following partial vs radical nephrectomy among older patients with early-stage kidney cancer
Abstract
Context: Although partial nephrectomy is the preferred treatment for many patients with early-stage kidney cancer, recent clinical trial data, which demonstrate better survival for patients treated with radical nephrectomy, have generated new uncertainty regarding the comparative effectiveness of these treatment options.
Objective: To compare long-term survival after partial vs radical nephrectomy among a population-based patient cohort whose treatment reflects contemporary surgical practice.
Design, setting, and patients: We performed a retrospective cohort study of Medicare beneficiaries with clinical stage T1a kidney cancer treated with partial or radical nephrectomy from 1992 through 2007. Using an instrumental variable approach to account for measured and unmeasured differences between treatment groups, we fit a 2-stage residual inclusion model to estimate the treatment effect of partial nephrectomy on long-term survival.
Main outcome measures: Overall and kidney cancer-specific survival.
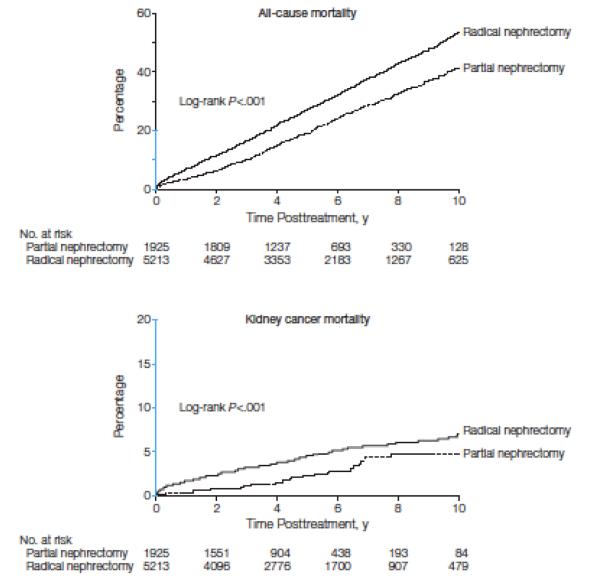
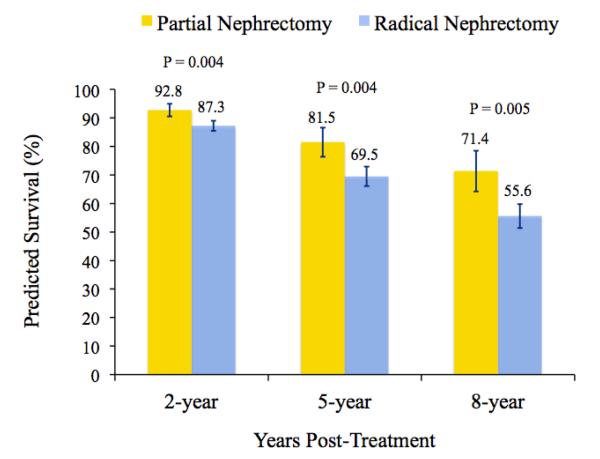
Results: Among 7138 Medicare beneficiaries with early-stage kidney cancer, we identified 1925 patients (27.0%) treated with partial nephrectomy and 5213 patients (73.0%) treated with radical nephrectomy. During a median follow-up of 62 months, 487 (25.3%) and 2164 (41.5%) patients died following partial or radical nephrectomy, respectively. Kidney cancer was the cause of death for 37 patients (1.9%) treated with partial nephrectomy, and 222 patients (4.3%) treated with radical nephrectomy. Patients treated with partial nephrectomy had a significantly lower risk of death (hazard ratio [HR], 0.54; 95% CI, 0.34-0.85). This corresponded with a predicted survival increase with partial nephrectomy of 5.6 (95% CI, 1.9-9.3), 11.8 (95% CI, 3.9-19.7), and 15.5 (95% CI, 5.0-26.0) percentage points at 2, 5, and 8 years posttreatment (P < .001). No difference was noted in kidney cancer-specific survival (HR, 0.82; 95% CI, 0.19-3.49).
Conclusion: Among Medicare beneficiaries with early-stage kidney cancer who were candidates for either surgery, treatment with partial rather than radical nephrectomy was associated with improved survival.
Figures
Comment in
-
Is it time for medicine-based evidence?JAMA. 2012 Apr 18;307(15):1641-3. doi: 10.1001/jama.2012.482. JAMA. 2012. PMID: 22511693 No abstract available.
-
Words of wisdom. Re: Long-term survival following partial vs radical nephrectomy among older patients with early-stage kidney cancer.Eur Urol. 2012 Aug;62(2):352-3. doi: 10.1016/j.eururo.2012.05.030. Eur Urol. 2012. PMID: 22748396 No abstract available.
-
Re: Long-term survival following partial vs radical nephrectomy among older patients with early-stage kidney cancer.J Urol. 2012 Nov;188(5):1723-4. doi: 10.1016/j.juro.2012.07.128. Epub 2012 Sep 19. J Urol. 2012. PMID: 23059212 No abstract available.
-
Commentary on "Long-term survival following partial vs. radical nephrectomy among older patients with early-stage kidney cancer." Tan HJ, Norton, EC, Ye Z, Hafez KS, Gore JL, Miller DC, Dow Division of Health Services Research, Department of Urology, University of Michigan, Ann Arbor, MI: JAMA 2012;307(15):1629-35.Urol Oncol. 2013 Jan;31(1):126-7. doi: 10.1016/j.urolonc.2012.11.004. Urol Oncol. 2013. PMID: 23419722
References
-
- Chow WH, Devesa SS, Warren JL, Fraumeni JF. Rising incidence of renal cell cancer in the United States. JAMA. 1999 May 5;281(17):1628–1631. - PubMed
-
- Hollingsworth JM, Miller DC, Daignault S, Hollenbeck BK. Rising incidence of small renal masses: a need to reassess treatment effect. JNCI. 2006 Sep 20;98(18):1331–1334. - PubMed
-
- Howlader N, Noone AM, Krapcho M, et al., editors. SEER Cancer Statistics Review, 1975-2008. National Cancer Institute; Bethesda, MD: [Accessed January 30, 2012]. Nov 10, 2011. http://seer.cancer.gov/csr/1975_2008/
-
- Fergany AF, Hafez KS, Novick AC. Long-term results of nephron sparing surgery for localized renal cell carcinoma: 10-year followup. J Urol. 2000 Feb;163(2):442–445. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
