

The association between skin blood flow and edema on epidermal thickness in the diabetic foot
- PMID: 22512286
- PMCID: PMC3389379
- DOI: 10.1089/dia.2011.0301
The association between skin blood flow and edema on epidermal thickness in the diabetic foot
Abstract
Background: Skin blood flow plays an important role in maintaining the health of the skin. The development of interstitial edema may impede oxygen diffusion to the skin. The aim of this study was to evaluate the association of skin blood flow and edema and epidermal thickness in the feet of people with and without diabetic neuropathy compared with a healthy control group.
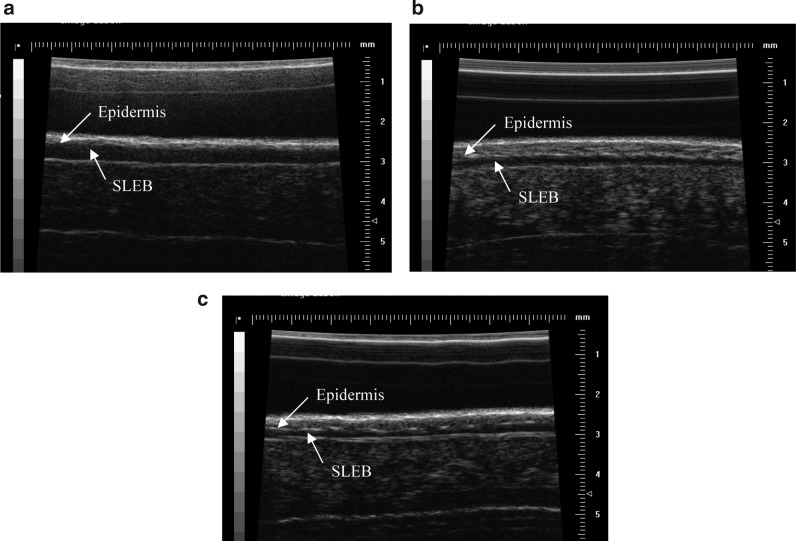
Subjects and methods: Eighty-seven subjects (19 people with diabetic neuropathy and foot ulceration, 35 people with diabetes but without neuropathy, and 33 healthy controls without diabetes) participated in the study. High-frequency ultrasonography was used to measure the epidermal thickness and edema in papillary skin at the big toe as reflected by the thickness of the subepidermal low echogenic band (SLEB). The capillary nutritive blood flow was measured by the use of video capillaroscopy, and skin blood flux was monitored by laser Doppler flowmetry.
Results: There was a 7.2% increase in epidermal thickness in those with diabetes but without neuropathy and a 16.5% decrease in people with diabetic neuropathy and foot ulceration compared with the healthy controls (all P<0.05). The SLEB thickness increased in all subjects with diabetes to a greater degree in those with neuropathy and ulceration than in those without (64.7% vs. 11.8%, P<0.001). Skin blood flux was shown to be higher in the diabetes groups than in the controls (all P<0.05), but no significant differences were found in the resting nutritive capillary blood flow (P>0.05). A significant negative correlation (P=0.002, r=-0.366) was demonstrated between the SLEB and epidermal thickness at the pulp of the big toe, whereas no significant correlation was demonstrated between skin blood flow and epidermal thickness (all P>0.05).
Conclusions: An increase in subepidermal edema was demonstrated in people with diabetic neuropathy and ulceration, which may partly contribute to reduced epidermal thickness at the pulp of the big toe. This may subsequently lead to the breaking down of skin in the diabetic foot.
Figures




References
-
- Mueller MJ. Zou D. Lott DJ. “Pressure gradient” as an indicator of plantar skin injury. Diabetes Care. 2005;28:2908–2912. - PubMed
-
- Bennett PJ. Stocks AE. Whittam DJ. Analysis of risk factors for neuropathic foot ulceration in diabetes mellitus. J Am Podiatr Med Assoc. 1996;86:112–116. - PubMed
-
- Fernando DJ. Masson EA. Veves A. Boulton AJ. Relationship of limited joint mobility to abnormal foot pressures and diabetic foot ulceration. Diabetes Care. 1991;14:8–11. - PubMed
-
- Zimny S. Dessel F. Ehren M. Pfohl M. Schatz H. Early detection of microcirculatory impairment in diabetic patients with foot at risk. Diabetes Care. 2001;24:1810–1814. - PubMed
-
- Urbancic-Rovan V. Stefanovska A. Bernjak A. Azman-Juvan K. Kocijancic A. Skin blood flow in the upper and lower extremities of diabetic patients with and without autonomic neuropathy. J Vasc Res. 2004;41:535–545. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
