

Whole brain radiotherapy for the treatment of newly diagnosed multiple brain metastases
- PMID: 22513917
- PMCID: PMC6457607
- DOI: 10.1002/14651858.CD003869.pub3
Whole brain radiotherapy for the treatment of newly diagnosed multiple brain metastases
Update in
-
Whole brain radiotherapy for the treatment of newly diagnosed multiple brain metastases.Cochrane Database Syst Rev. 2018 Jan 25;1(1):CD003869. doi: 10.1002/14651858.CD003869.pub4. Cochrane Database Syst Rev. 2018. PMID: 29365347 Free PMC article.
Abstract
Background: Brain metastases represent a significant healthcare problem. It is estimated that 20% to 40% of patients with cancer will develop metastatic cancer to the brain during the course of their illness. The burden of brain metastases impacts on quality and length of survival. Presenting symptoms include headache (49%), focal weakness (30%), mental disturbances (32%), gait ataxia (21%), seizures (18%), speech difficulty (12%), visual disturbance (6%), sensory disturbance (6%) and limb ataxia (6%).Brain metastases may spread from any primary site. The most common primary site is the lung, followed by the breast then gastrointestinal sites. Eighty-five per cent of brain metastases are found in the cerebral hemispheres, 10% to 15% in the cerebellum and 1% to 3% in the brainstem. Brain radiotherapy is used to treat cancer participants who have brain metastases from various primary malignancies.This is an update to the original review published in Issue 3, 2006.
Objectives: To assess the effectiveness and adverse effects of whole brain radiotherapy (WBRT) in adult participants with multiple metastases to the brain.
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL) (Issue 3, 2011), MEDLINE and EMBASE to July 2011.
Selection criteria: Randomized controlled trials (RCTs) comparing WBRT either alone or with other treatments in adults with newly diagnosed multiple metastases to the brain from any primary cancer. Trials of prophylactic WBRT were excluded as well as trials that dealt with surgery or WBRT, or both, for the treatment of single brain metastasis.
Data collection and analysis: Two review authors independently assessed trial quality and abstracted information. Adverse effects information was also collected from the trials.
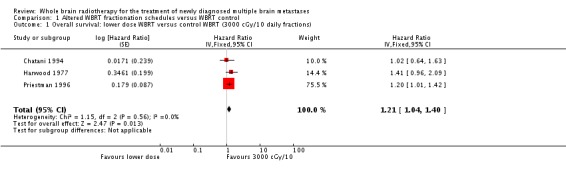
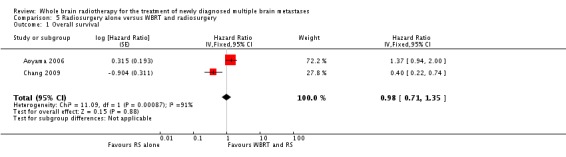
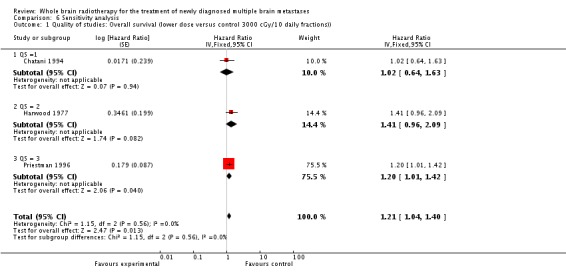
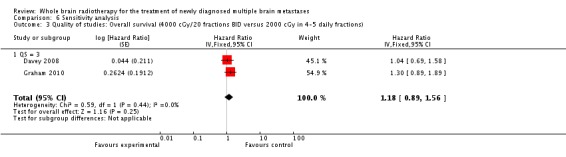
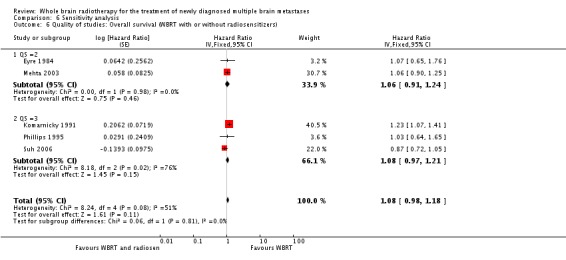
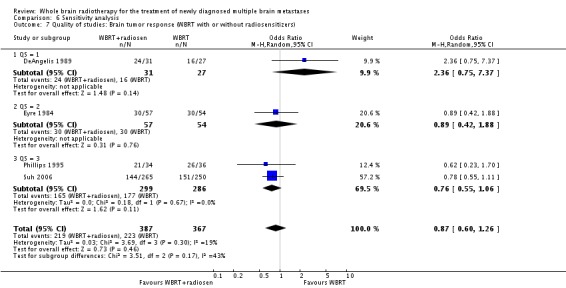
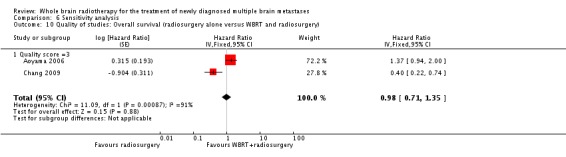
Main results: Nine RCTs involving 1420 participants were added in this updated review. This updated review now includes a total of 39 trials involving 10,835 participants.Eight published reports (nine RCTs) showed no benefit of altered dose-fractionation schedules as compared to the control fractionation (3000 cGy in 10 fractions daily) of WBRT for overall survival. These studies also showed no improvement in symptom control nor neurologic improvement among the different dose-fractionation schemes as compared to 3000 cGy in 10 daily fractions of WBRT. This updated review includes two trials comparing 4000 cGy in 20 fractions given twice daily versus 2000 cGy in 4 or 5 daily fractions. Overall, there was no survival advantage (hazard ratio (HR) 1.18, 95% confidence interval (CI) 0.89 to 1.56, P = 0.25) with the use of 4000 cGy in 20 fractions given twice daily compared to 2000 cGy in 4 or 5 daily fractions.The addition of radiosensitizers in six RCTs did not confer additional benefit to WBRT in either the overall survival times (HR 1.08, 95% CI 0.98 to 1.18, P = 0.11) or brain tumour response rates (HR 0.87, 95% CI 0.60 to 1.26, P = 0.46).Two RCTs found no benefit in overall survival (HR 0.61, 95% CI 0.27 to 1.39, P = 0.24) with the use of WBRT and radiosurgery boost as compared to WBRT alone for selected participants with multiple brain metastases (up to four brain metastases). Overall, there was a statistically significant improvement in local brain control (HR 0.35, 95% CI 0.20 to 0.61, P = 0.0003) favouring the WBRT and radiosurgery boost arm. Only one trial of radiosurgery boost with WBRT reported an improved Karnofsky performance score outcome and improved ability to reduce the dexamethasone dose.In this updated review, a total of three RCTs reported on selected patients (with up to three or four brain metastases) treated with radiosurgery alone versus WBRT and radiosurgery. Based on two trials, there was no difference in overall survival (HR 0.98, 95% CI 0.71 to 1.35, P = 0.88). The addition of WBRT when added to radiosurgery significantly improved locally treated brain metasatases control (HR 2.61, 95% CI 1.68 to 4.06, P < 0.0001) and distant brain control (HR 2.15, 95% CI 1.55 to 2.99, P < 0.00001). On the other hand, one trial concluded that patients treated with WBRT and radiosurgery boost were significantly more likely to show a decline in learning and memory function as compared to those treated with radiosurgery alone.One RCT examined the use of WBRT and prednisone versus prednisone alone and produced inconclusive results.
Authors' conclusions: None of the RCTs with altered WBRT dose-fractionation schemes as compared to standard (3000 cGy in 10 daily fractions or 2000 cGy in 4 or 5 daily fractions) found a benefit in terms of overall survival, neurologic function, or symptom control.The use of radiosensitizers or chemotherapy in conjunction with WBRT remains experimental.Radiosurgery boost with WBRT may improve local disease control in selected participants as compared to WBRT alone, although survival remains unchanged for participants with multiple brain metastases.This updated review now includes a total of three RCTs examining the use of radiosurgery alone versus WBRT and radiosurgery. The addition of WBRT to radiosurgery improves local and distant brain control but there is no difference in overall survival. Patients treated with radiosurgery alone were found to have better neurocognitive outcomes in one trial as compared to patients treated with WBRT and radiosurgery.The benefit of WBRT as compared to supportive care alone has not been studied in RCTs. It may be that supportive care alone, without WBRT, is appropriate for some participants, particularly those with advanced disease and poor performance status.
Conflict of interest statement
None known
Figures

















Update of
-
Whole brain radiotherapy for the treatment of multiple brain metastases.Cochrane Database Syst Rev. 2006 Jul 19;(3):CD003869. doi: 10.1002/14651858.CD003869.pub2. Cochrane Database Syst Rev. 2006. Update in: Cochrane Database Syst Rev. 2012 Apr 18;(4):CD003869. doi: 10.1002/14651858.CD003869.pub3. PMID: 16856022 Updated.
References
References to studies included in this review
-
- Andrews DW, Scott CB, Sperduto PW, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet 2004;363:1665‐72. - PubMed
-
- Antonadou D, Coliarakis N, Paraskevaidis M, Athansiou H, Sarris G, Synodinou M, et al. Whole brain radiotherapy alone or in combination with temozolamide for brain metastases. A phase III study (abstract). International Journal of Radiation Oncology, Biology, Physics 2002;54:93.
-
- Aoyama H, Shirato H, Tago M, et al. Stereotactic radiosurgery plus whole‐brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases. A randomized controlled trial. JAMA 2006;295(21):2483‐91. - PubMed
-
- Borgelt B, Gelber R, Kramer S, Brady LW, Chang CH, Davis LW, et al. The palliation of brain metastases: final results of the first two studies by the Radiation Therapy Oncology Group. International Journal of Radiation Oncology, Biology, Physics 1980;6:1‐9. - PubMed
-
- Borgelt B, Gelber R, Kramer S, et al. The palliation of brain metastases: final results of the first two studies by the Radiation Therapy Oncology Group. International Journal of Radiation Oncology, Biology, Physics 1980;6:1‐9. - PubMed
References to studies excluded from this review
-
- Haie‐Meder C, Pellae‐Cosset B, Laplanche A, Lagrange JL, Tuchais C, Nogues C, et al. Results of a randomized clinical trial comparing two radiation schedules in the palliative treatment of brain metastases. Radiotherapy and Oncology 1993;26:111‐6. - PubMed
References to ongoing studies
-
- Phase III randomized study of radiosurgery with or without WBRT in patients with one to three cerebral metastases. Ongoing study Starting date of trial not provided. Contact author for more information.
-
- NCI‐P02‐0211 Phase III randomized study of d‐methylphenidate to improve quality of life in patients receiving radiotherapy for primary or metastatic brain tumours. Ongoing study Starting date of trial not provided. Contact author for more information.
-
- Phase III randomized study of temozolomide with or without WBRT in patients with stage IV melanoma with asymptomatic brain metastases. Ongoing study Closed.
-
- Protocol ID: 040066 Surgery versus radiosurgery to treat metastatic brain tumors. Ongoing study Starting date of trial not provided. Contact author for more information.
-
- Protocol ID: P03247 Temozolomide for treatment of brain metastases from non‐small cell lung cancer. Ongoing study Starting date of trial not provided. Contact author for more information.
Additional references
-
- Arbit E, Wronski M. The treatment of brain metastases. Neurosurgery Quarterly 1995;5:1.
-
- Cairncross JG, Kim JH, Posner JB. Radiation therapy for brain metastases. Annals of Neurology 1980;7:529‐41. - PubMed
-
- Chao JH, Philips R, Nickson JJ. Roentgen ray therapy for cerebral metastases. Cancer 1954;7:682‐9. - PubMed
-
- Detsky AS, Naylor CD, O'Rourke K, McGeer AJ, L'Abbe KA. Incorporating variations in the quality of individual randomized trials into meta‐analysis. Journal of Clinical Epidemiology 1992;45:255‐65. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical