

Case Reports
doi: 10.1259/bjr/92343528.
Epub 2012 Apr 18.
Imaging manifestations in Proteus syndrome: an unusual multisystem developmental disorder
Affiliations
- PMID: 22514103
- PMCID: PMC3487101
- DOI: 10.1259/bjr/92343528
Item in Clipboard
Case Reports
Imaging manifestations in Proteus syndrome: an unusual multisystem developmental disorder
Br J Radiol.
2012 Sep.
Abstract
In this review we use images from an 11-year-old male to describe Proteus syndrome, a complex disorder with multisystem involvement and great clinical variability. Our aim is to enhance recognition of the typical imaging findings, which can aid diagnosis of this rare condition.
Figures

Subcutaneous fat hypertrophy on the left anterior chest wall (arrow).
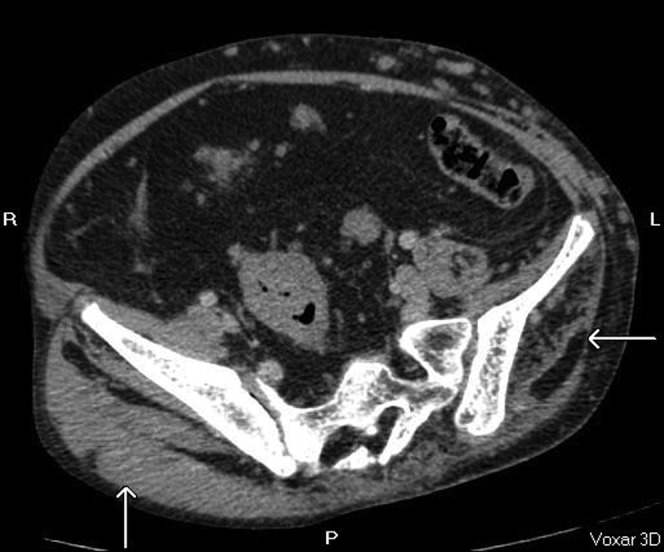
Asymmetrical atrophy of the left gluteal muscles with fatty infiltration
(arrow).
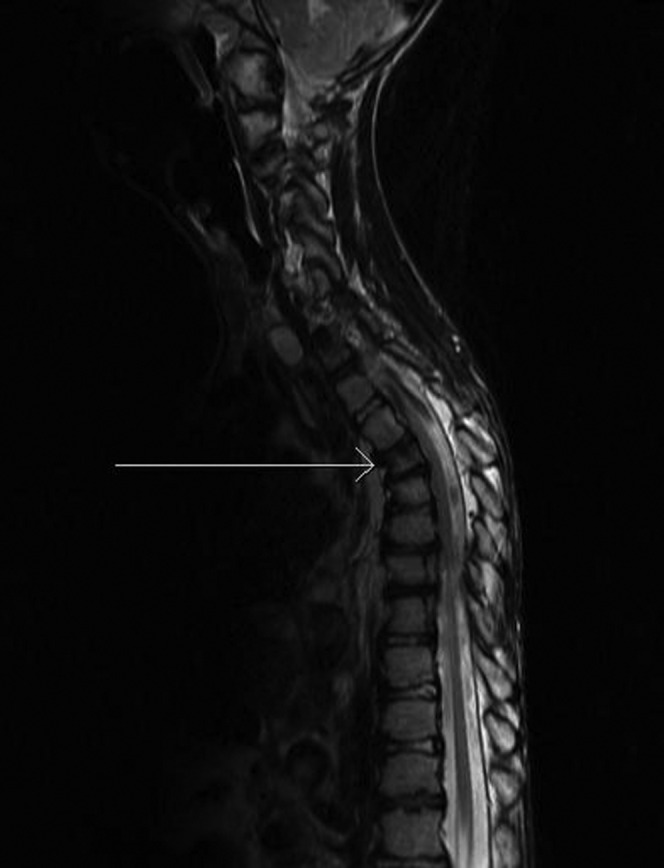
Loss of T4 vertebral body height (arrow).

Kyphoscoliosis of the upper thoracic vertebrae (arrow) (axial CT bone windows).

Lateral X-ray of the foot in an 11-year-old male, demonstrating soft tissue
overgrowth in keeping with plantar cerebriform connective tissue naevus. The
metatarsals are osteopenic, gracile and overtubulated with widened joint spaces.
Degenerative changes from the gross deformities are noted in the tibiocalcaneal
joint.

Anteroposterior view demonstrates absence of distal end of the first metatarsal
distal phalanx (arrow).

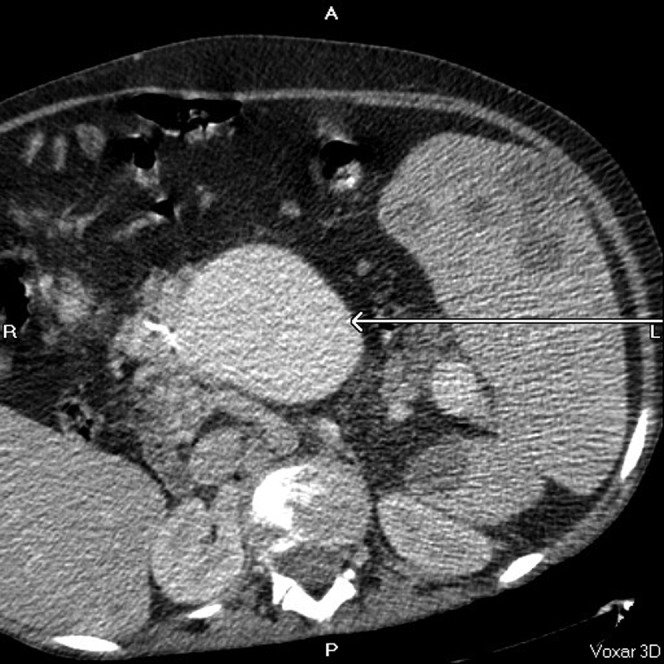
Ectactic confluence of splenic (central arrow) and portal vein (arrow to
the left of the image) with varicosities at the hila (axial CT, post-contrast
portal venous phase).
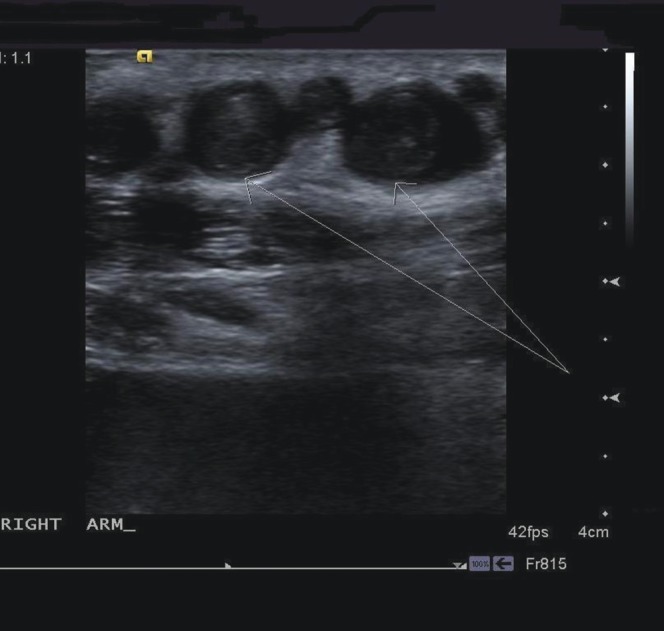
Transverse ultrasound images through right forearm demonstrating enlarged
peripheral veins with thrombus (arrows) within.

Inferior vena cava (arrow); Figures
10–14 show interval imaging on the same patient, demonstrating
progression of the vascular abnormalities.

Dilated superior mesenteric vein (arrow).
Subcutaneous collateral vessels (arrows).
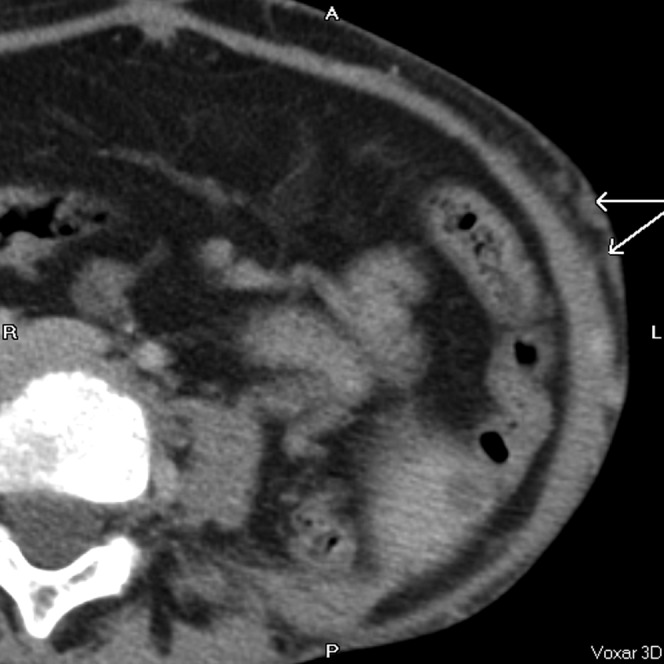
Gross aneurysmal enlargement of the inferior vena cava (lower arrow to
the left of the image) and internal mammary vessels (upper arrow to the right
of the image).
Superior mesenteric vein (arrow).

Enlarged subcutaneous collateral vessels (arrows).

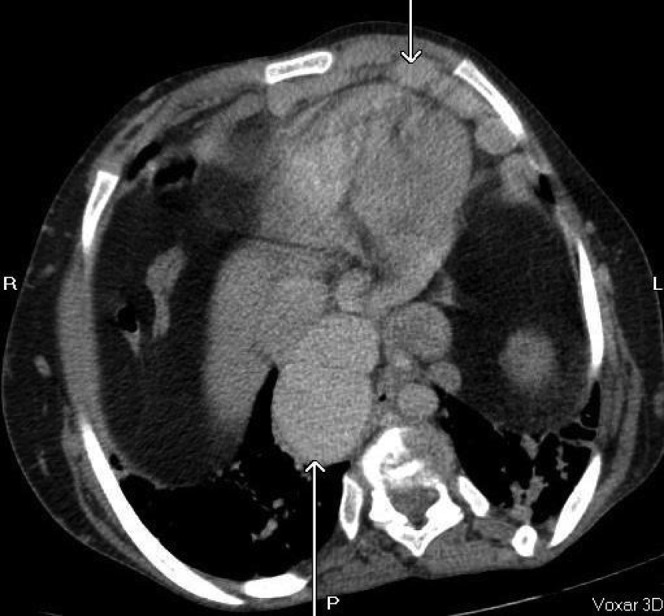
Massive splenomegaly (30 cm) with multiple splenic cysts (arrows), some
of which have soft tissue components within. Coronal, axial and sagittal post-contrast
CT images.
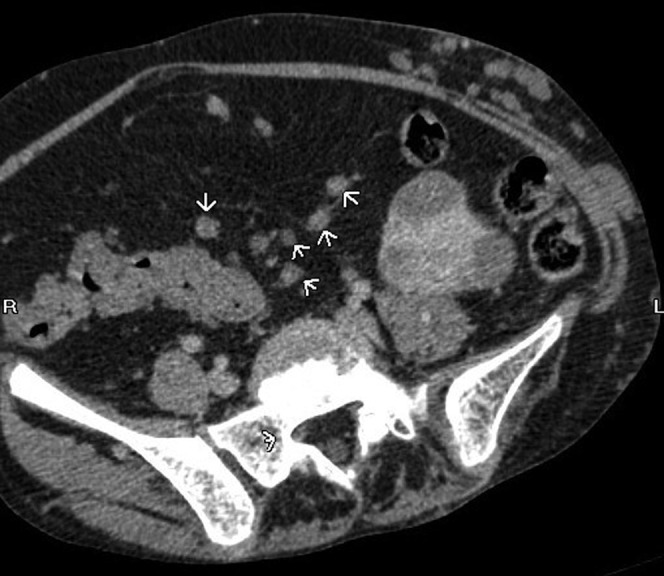
Peritoneal lymphatic nodules (arrowheads). Coronal, axial and sagittal
post-contrast CT images.
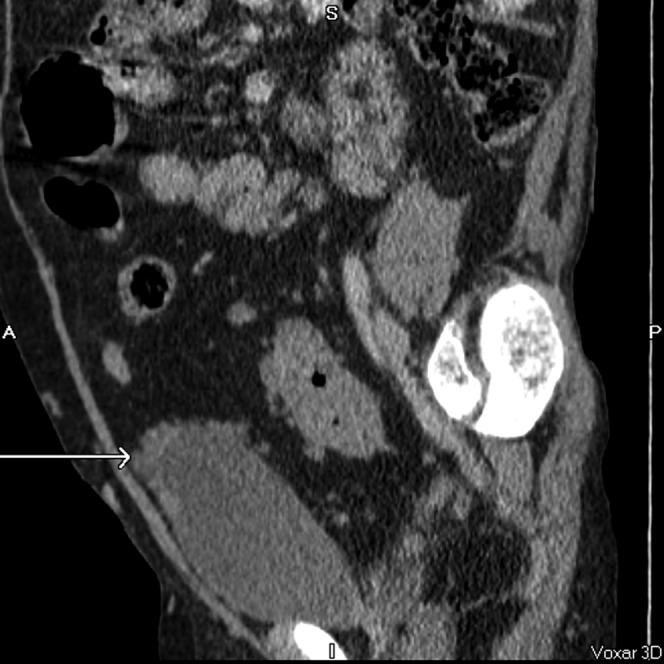
Multiple nodules around the bladder dome (arrow) creating spurious appearance
of nodular bladder wall thickening. Coronal, axial and sagittal post-contrast
CT images.

Emphysematous changes with bullae formation (arrow). Axial CT, lung windows.
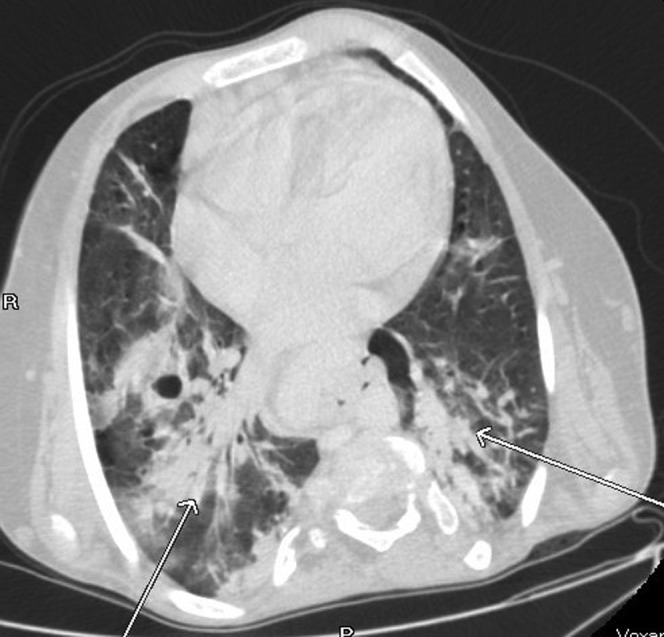
Extensive bibasal consolidation (arrows). This has not been reported as
a common finding. The patient was admitted with non-specific abdominal pain
and there were no clinical or biochemical features to suggest pneumonia. Axial
CT, lung windows.
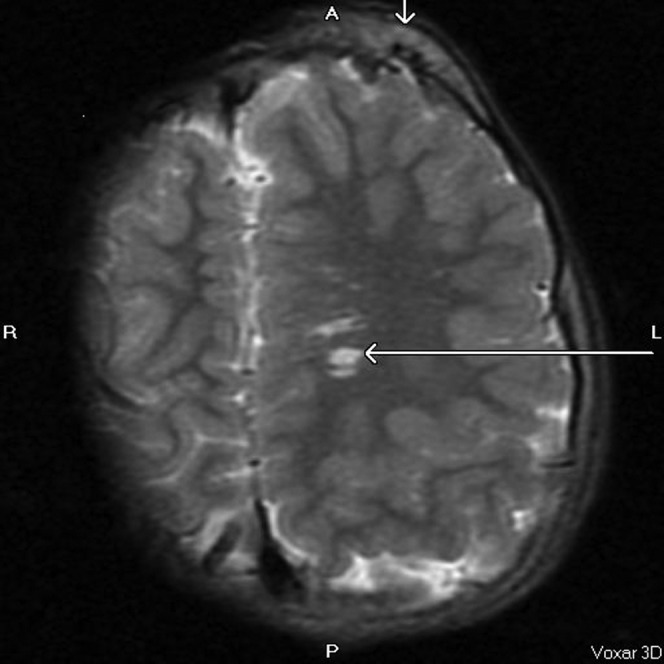
Asymmetrical calvarial thickening (vertical arrow) and arteriovenous malformation
(horizontal arrow). MRI image, axial T2, repetition
time 5700 ms, echo time 98 ms.
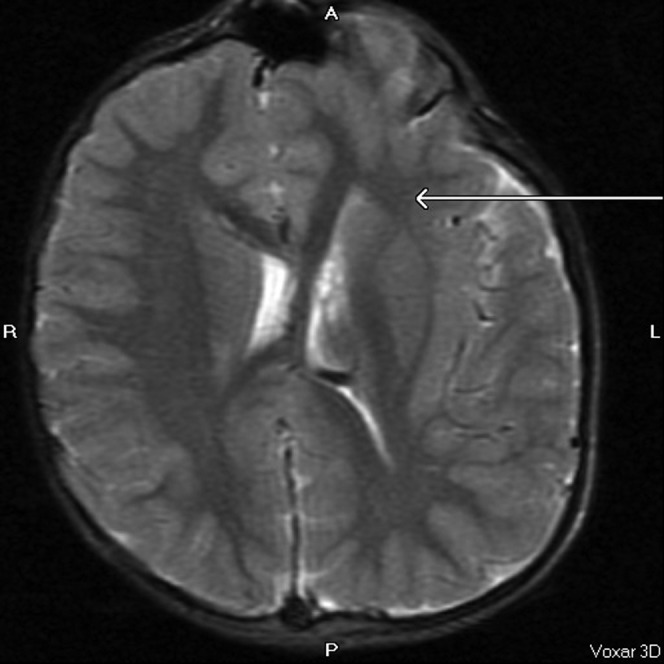
Asymmetry of the cerebral hemispheres and lateral ventricles with abnormal
grey–white matter differentiation (arrow) and areas of macrogyria in
the left cerebral hemisphere. MRI image, axial T2,
repetition time 5700 ms, echo time 98 ms.
References
-
- Cohen MM, Jr, Hayden PW. A newly recognized hamartomatous syndrome. Birth Defects Orig Artic Ser 1979;15:291–6 - PubMed
-
- Wiedemann H-R, Burgio GR, Aldenhoff P, Kunze J, Kaufmann HJ, Schirg E. The Proteus syndrome: partial gigantism of the hands and/or feet, nevi, hemihypertrophy, subcutaneous tumors, macrocephaly or other skull anomalies and possible accelerated growth and visceral affections. Eur J Pediatr 1983;140:5–12 - PubMed
-
- Friedman LD. Medicine and the arts. The elephant man. Acad Med 2000;75:448–9 - PubMed
-
- Biesecker LG, Happle R, Mulliken JB, Weksberg R, Graham JM, Jr, Viljoen DL, et al. Proteus syndrome: diagnostic criteria, differential diagnosis, and patient evaluation. Am J Med Genet 1999;84:389–95 - PubMed
-
- Jamis-Dow CA, Turner J, Biesecker LG, Choyke PL. Radiologic manifestations of Proteus syndrome. RadioGraphics 2004;24:1051–68 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
