

Recursive partitioning analysis of prognostic factors for glioblastoma patients aged 70 years or older
- PMID: 22517216
- PMCID: PMC3402652
- DOI: 10.1002/cncr.27570
Recursive partitioning analysis of prognostic factors for glioblastoma patients aged 70 years or older
Abstract
Background: The most-used prognostic scheme for malignant gliomas included only patients aged 18 to 70 years. The purpose of this study was to develop a prognostic model for patients ≥70 years of age with newly diagnosed glioblastoma.
Methods: A total of 437 patients ≥70 years of age with newly diagnosed glioblastoma, pooled from 2 tertiary academic institutions, was identified for recursive partitioning analysis (RPA). The resulting prognostic model, based on the final pruned RPA tree, was validated using 265 glioblastoma patients ≥70 years of age from a data set independently compiled by a French consortium.
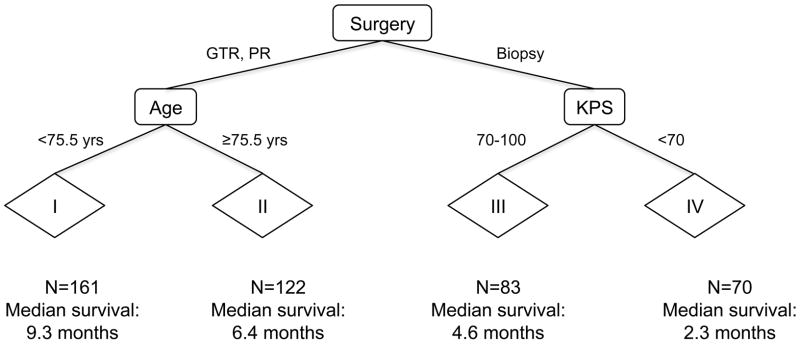
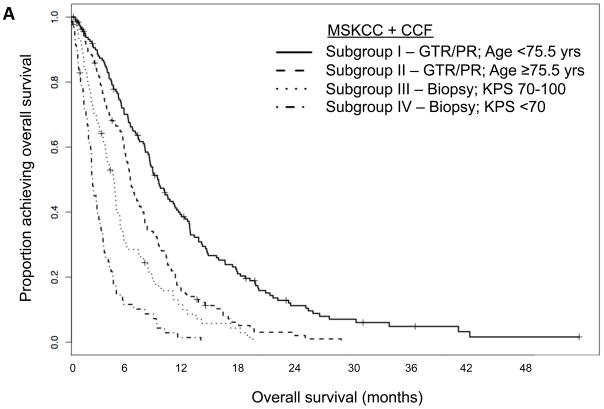
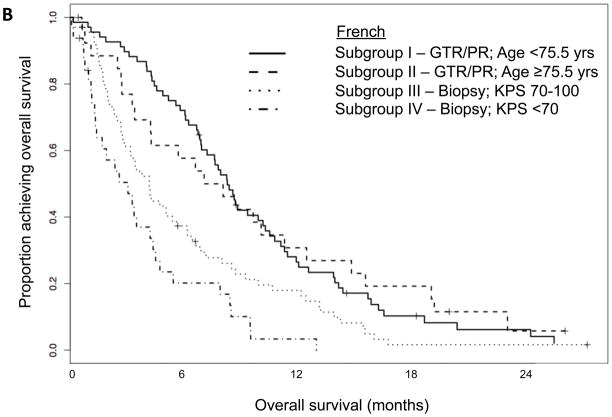
Results: RPA produced 9 terminal nodes, which were pruned to 4 prognostic subgroups with markedly different median survivals: subgroup I = patients <75.5 years of age who underwent surgical resection (9.3 months); subgroup II = patients ≥75.5 years of age who underwent surgical resection (6.4 months); subgroup III = patients with Karnofsky performance status of 70 to 100 who underwent biopsy only (4.6 months); and subgroup IV = patients with Karnofsky performance status <70 who underwent biopsy only (2.3 months). Application of this prognostic model to the French cohort also resulted in significantly different (P < .0001) median survivals for subgroups I (8.5 months), II (7.7 months), III (4.3 months), and IV (3.1 months).
Conclusions: This model divides elderly glioblastoma patients into prognostic subgroups that can be easily implemented in both the patient care and the clinical trial settings. This purely clinical prognostic model serves as a backbone for the future incorporation of the increasing number of potential molecular prognostic markers.
Copyright © 2012 American Cancer Society.
Figures
References
-
- Wen PY, Kesari S. Malignant gliomas in adults. N Engl J Med. 2008;359(5):492–507. - PubMed
-
- Fisher JL, Schwartzbaum JA, Wrensch M, Wiemels JL. Epidemiology of brain tumors. Neurol Clin. 2007;25(4):867–890. vii. - PubMed
-
- Batchelor TT, Betensky RA, Esposito JM, et al. Age-dependent prognostic effects of genetic alterations in glioblastoma. Clin Cancer Res. 2004;10(1 Pt 1):228–233. - PubMed
-
- Nobusawa S, Watanabe T, Kleihues P, Ohgaki H. IDH1 mutations as molecular signature and predictive factor of secondary glioblastomas. Clin Cancer Res. 2009;15(19):6002–6007. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
