

Total hip arthroplasty versus resurfacing arthroplasty in the treatment of patients with arthritis of the hip joint: single centre, parallel group, assessor blinded, randomised controlled trial
- PMID: 22517930
- PMCID: PMC3330050
- DOI: 10.1136/bmj.e2147
Total hip arthroplasty versus resurfacing arthroplasty in the treatment of patients with arthritis of the hip joint: single centre, parallel group, assessor blinded, randomised controlled trial
Abstract
Objectives: To compare the clinical and cost effectiveness of total hip arthroplasty with resurfacing arthroplasty in patients with severe arthritis of the hip.
Design: Single centre, two arm, parallel group, assessor blinded, randomised controlled trial with 1:1 treatment allocation.
Setting: One large teaching hospital in the United Kingdom.
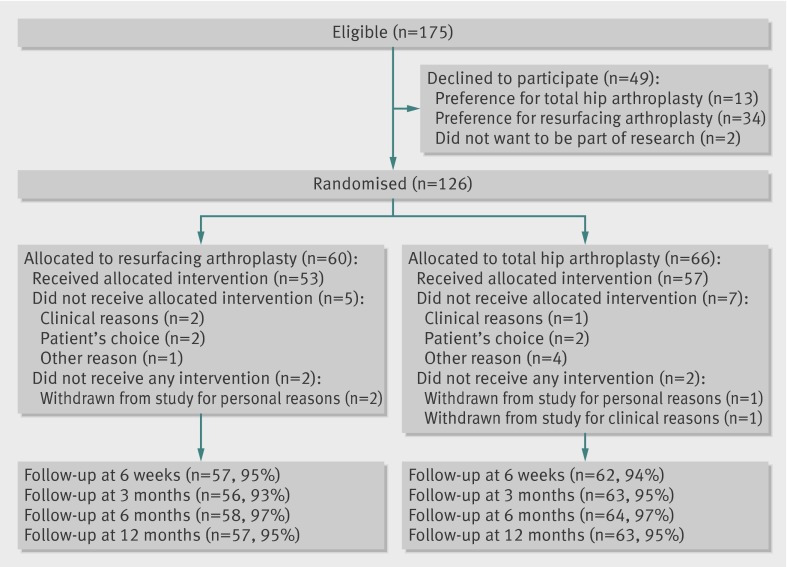
Participants: 126 patients older than 18 years with severe arthritis of the hip joint, suitable for resurfacing arthroplasty of the hip. Patients were excluded if they were considered to be unable to adhere to trial procedures or complete questionnaires.
Interventions: Total hip arthroplasty (replacement of entire femoral head and neck); hip resurfacing arthroplasty (replacement of the articular surface of femoral head only, femoral neck remains intact). Both procedures replaced the articular surface of the acetabulum.
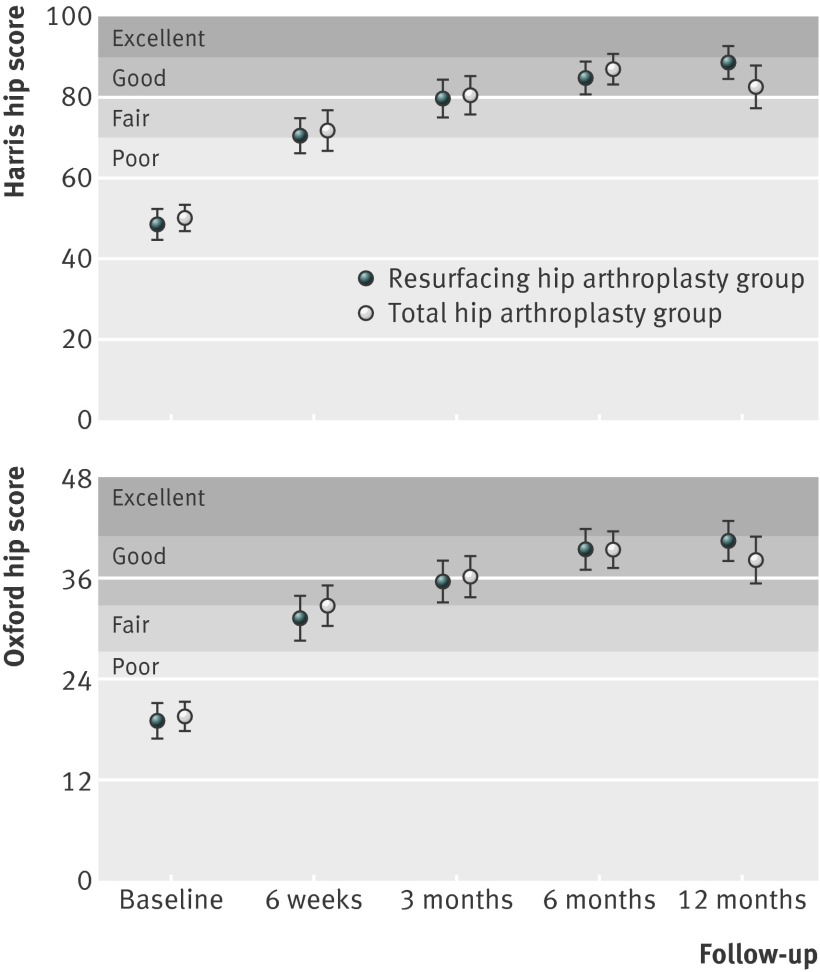
Main outcome measures: Hip function at 12 months after surgery, assessed using the Oxford hip score and Harris hip score. Secondary outcomes were quality of life, disability rating, physical activity level, complications, and cost effectiveness.
Results: 60 patients were randomly assigned to hip resurfacing arthroplasty and 66 to total hip arthroplasty. Intention to treat analysis showed no evidence for a difference in hip function between treatment groups at 12 months (t test, P=0.242 and P=0.070 for Oxford hip score and Harris hip score, respectively); 95% of follow-up data was available for analysis. Mean Oxford hip score was 40.4 (95% confidence interval 37.9 to 42.9) in the resurfacing group and 38.2 (35.3 to 41.0) in the total arthroplasty group (estimated treatment effect size 2.23 (-1.52 to 5.98)). Mean Harris hip score was 88.4 (84.4 to 92.4) in the resurfacing group and 82.3 (77.2 to 87.5) in the total arthroplasty group (6.04 (-0.51 to 12.58)). Although we saw no evidence of a difference, we cannot definitively exclude clinically meaningful differences in hip function in the short term. Overall complication rates did not differ between treatment groups (P=0.291). However, we saw more wound complications in the total arthroplasty group (P=0.056) and more thromboembolic events in the resurfacing group (P=0.049).
Conclusions: No evidence of a difference in hip function was seen in patients with severe arthritis of the hip, one year after receiving a total hip arthroplasty versus resurfacing arthroplasty. The long term effects of these interventions remain uncertain.
Trial registration: Current Controlled Trials ISRCTN33354155, UKCRN 4093.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Hip resurfacing or stemmed arthroplasty for young active patients?BMJ. 2012 Apr 19;344:e2663. doi: 10.1136/bmj.e2663. BMJ. 2012. PMID: 22517931 No abstract available.
-
Study lacks rigour to determine choice of hip resurfacing or arthroplasty.BMJ. 2012 May 28;344:e3667; author reply e3672. doi: 10.1136/bmj.e3667. BMJ. 2012. PMID: 22641800 No abstract available.
References
-
- Murray DW, Carr AJ, Bulstrode CJ. Which primary total hip replacement? J Bone Joint Surg Br 1995;77:520-7. - PubMed
-
- Wroblewski BM, Fleming PA, Siney PD. Charnley low-frictional torque arthroplasty of the hip. 20-to-30 year results. J Bone Joint Surg Br 1999;81:427-30. - PubMed
-
- Digas G, Karrholm J, Thanner J, Malchau H, Herberts P. The Otto Aufranc Award. Highly cross-linked polyethylene in total hip arthroplasty: randomized evaluation of penetration rate in cemented and uncemented sockets using radiostereometric analysis. Clin Orthop Relat Res 2004;429:6-16. - PubMed
-
- Grigoris P, Roberts P, Panousis K, Jin Z. Hip resurfacing arthroplasty: the evolution of contemporary designs. Proc Inst Mech Eng H 2006;220:95-105. - PubMed
-
- Australian National Joint Replacement Registry. Demographics of hip and knee arthroplasty. 2010. www.dmac.adelaide.edu.au/aoanjrr/documents/aoanjrrreport_2010.pdf.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical