

Antenatal bartter syndrome: a review
- PMID: 22518185
- PMCID: PMC3299276
- DOI: 10.1155/2012/857136
Antenatal bartter syndrome: a review
Abstract
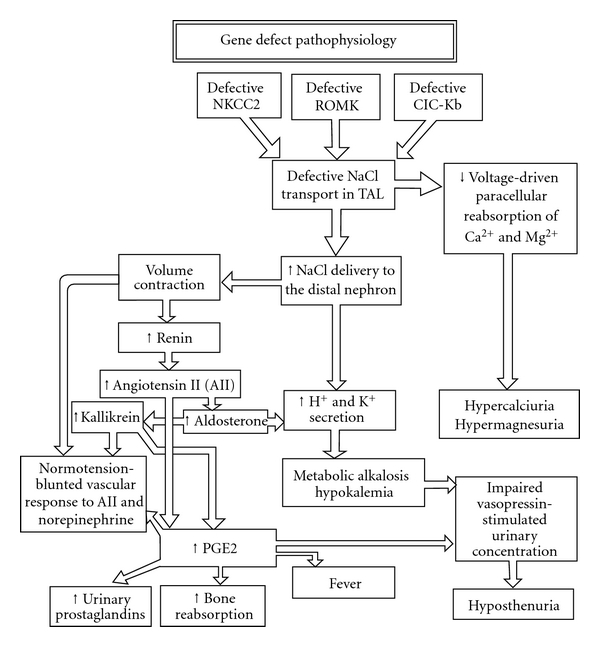
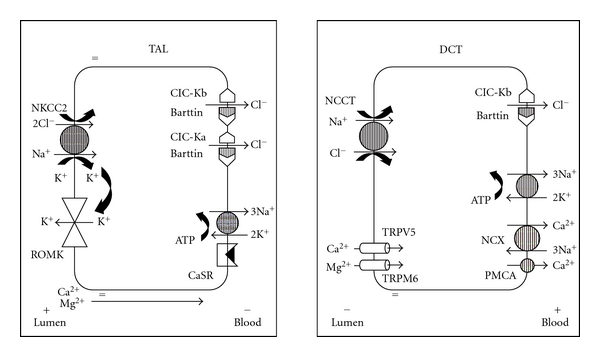
Antenatal Bartter syndrome (ABS) is a rare autosomal recessive renal tubular disorder. The defective chloride transport in the loop of Henle leads to fetal polyuria resulting in severe hydramnios and premature delivery. Early onset, unexplained maternal polyhydramnios often challenges the treating obstetrician. Increasing polyhydramnios without apparent fetal or placental abnormalities should lead to the suspicion of this entity. Biochemical analysis of amniotic fluid is suggested as elevated chloride level is usually diagnostic. Awareness, early recognition, maternal treatment with indomethacin, and amniocentesis allow the pregnancy to continue. Affected neonates are usually born premature, have postnatal polyuria, vomiting, failure to thrive, hypercalciuria, and subsequently nephrocalcinosis. Hypokalemia, metabolic alkalosis, secondary hyperaldosteronism and hyperreninaemia are other characteristic features. Volume depletion due to excessive salt and water loss on long term stimulates renin-angiotensin-aldosterone system resulting in juxtaglomerular hyperplasia. Clinical features and electrolyte abnormalities may also depend on the subtype of the syndrome. Prenatal diagnosis and timely indomethacin administration prevent electrolyte imbalance, restitute normal growth, and improve activity. In this paper, authors present classification, pathophysiology, clinical manifestations, laboratory findings, complications, and prognosis of ABS.
Figures
References
-
- Bartter FC, Pronove P, Gill JR, Jr., MacCardle RC. Hyperplasia of the juxtaglomerular complex with hyperaldosteronism and hypokalemic alkalosis. A new syndrome. American Journal of Medicine. 1962;33:811–828. - PubMed
-
- Dell KM, Avner ED. Bartter-Gitelman syndromes and other inherited tubular transport abnormalities. In: Kleigman RM, Behrman RE, Jenson HB, Stanton BF, editors. Nelson Textbook of Pediatrics. 18th edition. Philadelphia, Pa, USA: Saunders; 2007. pp. 2201–2202.
-
- Proesmans W. Bartter syndrome and its neonatal variant. European Journal of Pediatrics. 1997;156(9):669–679. - PubMed
-
- Bhat YR, Vinayaka G, Vani R, Prashanth KA, Sreelakshmi K. Antenatal Bartter syndrome: a rare cause of unexplained severe polyhydramnios. Annals of Tropical Paediatrics. 2011;31:153–157. - PubMed
-
- Brochard K, Boyer O, Blanchard A, et al. Phenotype-genotype correlation in antenatal and neonatal variants of Bartter syndrome. Nephrology Dialysis Transplantation. 2009;24(5):1455–1464. - PubMed
LinkOut - more resources
Full Text Sources
