

Evaluation of shock wave lithotripsy injury in the pig using a narrow focal zone lithotriptor
- PMID: 22519983
- PMCID: PMC3405199
- DOI: 10.1111/j.1464-410X.2012.11160.x
Evaluation of shock wave lithotripsy injury in the pig using a narrow focal zone lithotriptor
Abstract
What's known on the subject? and What does the study add? Of all the SW lithotriptors manufactured to date, more research studies have been conducted on and more is known about the injury (both description of injury and how to manipulate injury size) produced by the Dornier HM-3 than any other machine. From this information have come suggestions for treatment protocols to reduce shock wave (SW)-induced injury for use in stone clinics. By contrast, much less is known about the injury produced by narrow-focus and high-pressure lithotriptors like the Storz Modulith SLX. In fact, a careful study looking at the morphology of the injury produced by the SLX itself is lacking, as is any study exploring ways to reduce renal injury by manipulating SW delivery variables of this lithotriptor. The present study quantitates the lesion size and describes the morphology of the injury produced by the SLX. In addition, we report that reducing the SW delivery rate, a manoeuvre known to lower injury in the HM-3, does not reduce lesion size in the SLX.
Objective: • To assess renal injury in a pig model after treatment with a clinical dose of shock waves using a narrow focal zone (≈3 mm) lithotriptor (Modulith SLX, Karl Storz Lithotripsy).
Materials and methods: • The left kidney of anaesthetized female pigs were treated with 2000 or 4000 shock waves (SWs) at 120 SWs/min, or 2000 SWs at 60 SWs/min using the Storz SLX. • Measures of renal function (glomerular filtration rate and renal plasma flow) were collected before and 1 h after shock wave lithotripsy (SWL) and the kidneys were harvested for histological analysis and morphometric quantitation of haemorrhage in the renal parenchyma with lesion size expressed as a percentage of functional renal volume (FRV). • A fibre-optic probe hydrophone was used to determine acoustic output and map the focal width of the lithotriptor. • Data for the SLX were compared with data from a previously published study in which pigs of the same age (7-8 weeks) were treated (2000 SWs at 120 or 60 SWs/min) using an unmodified Dornier HM3 lithotriptor.
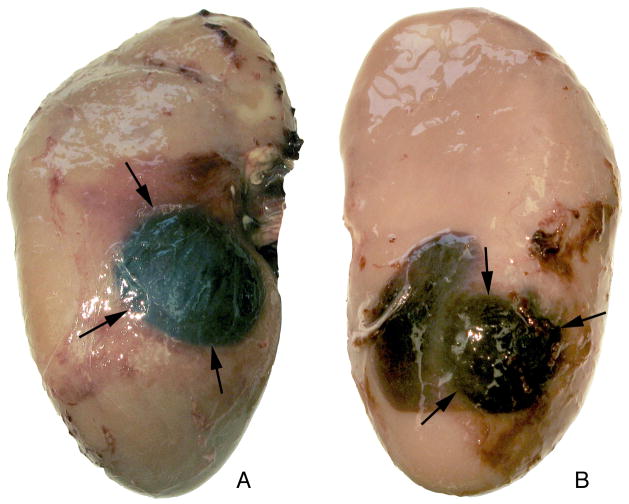
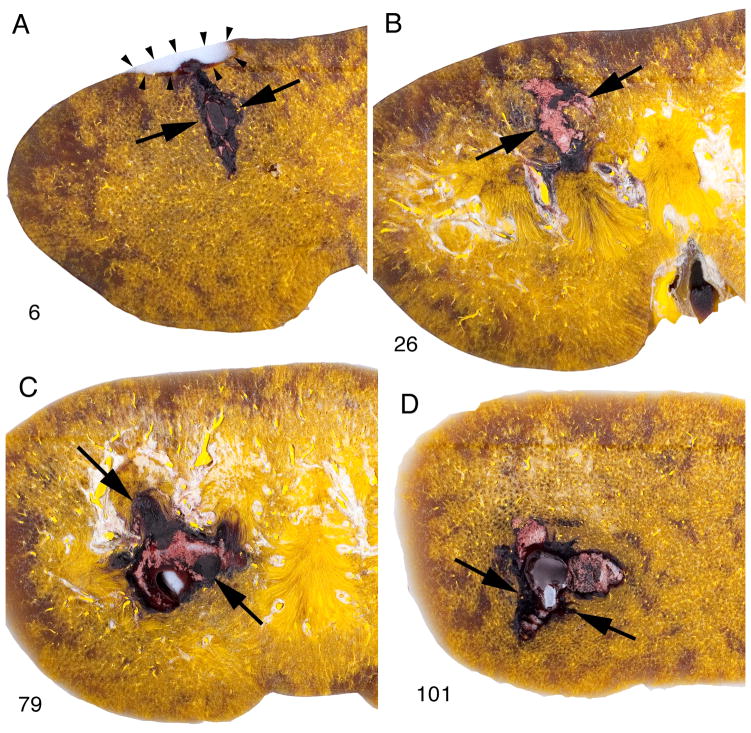
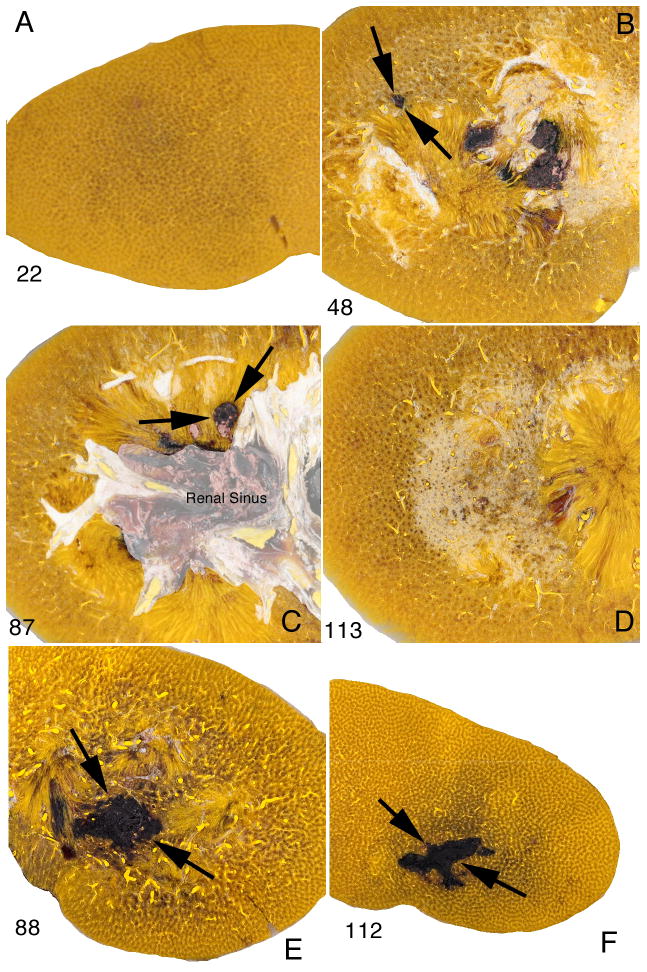
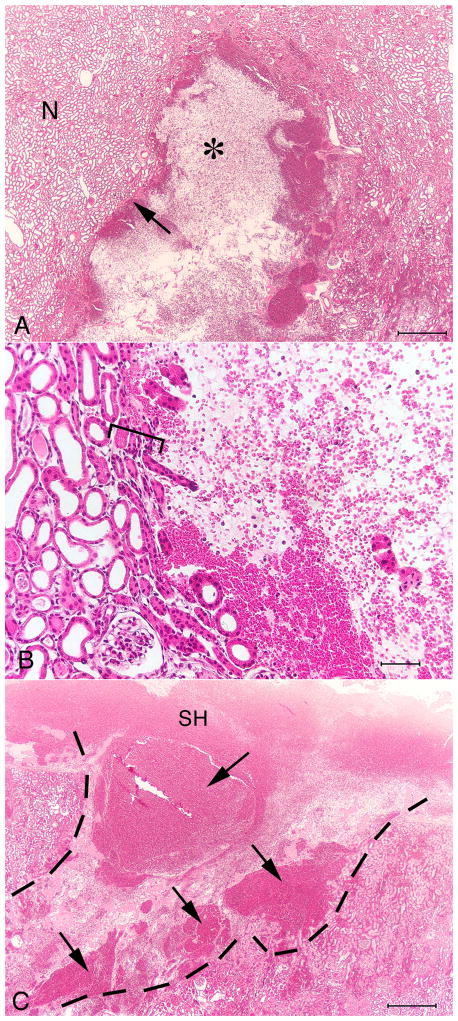
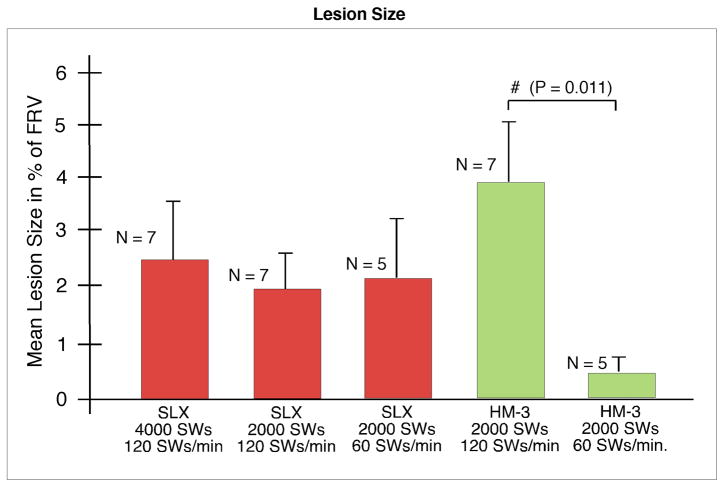
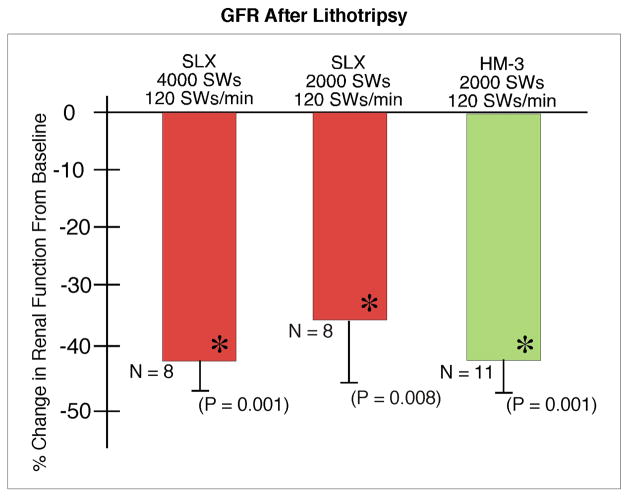
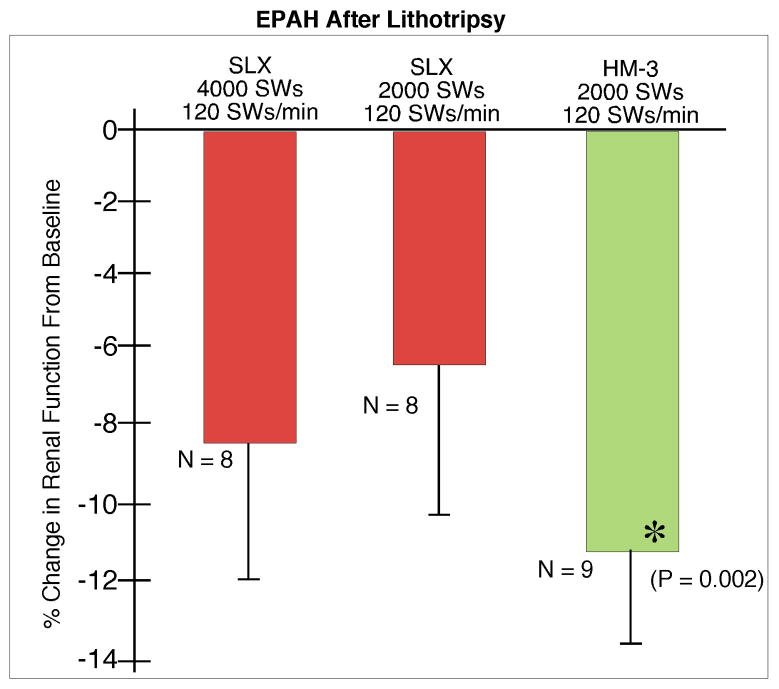
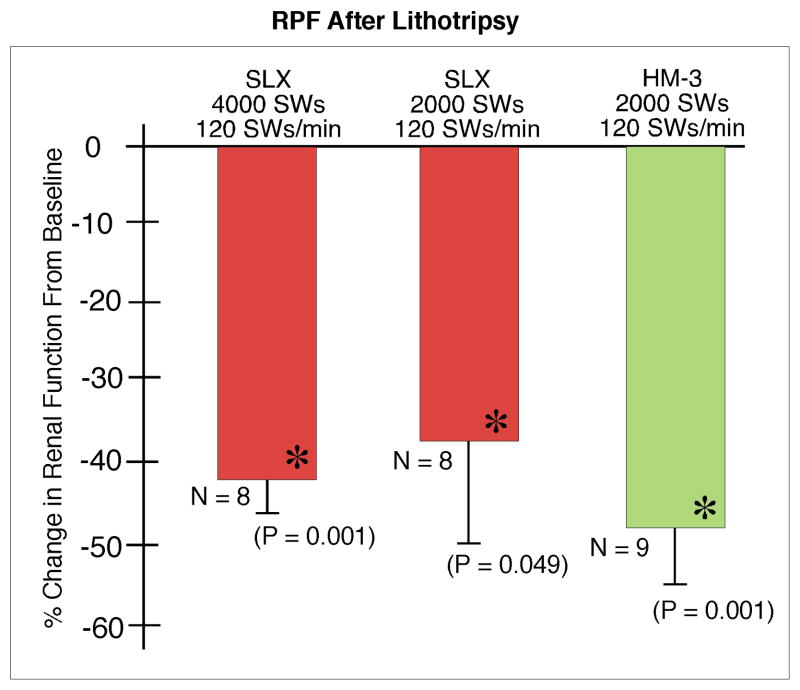
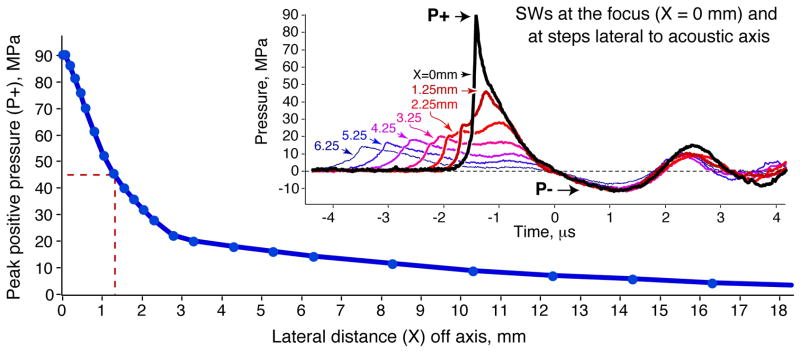
Results: • Treatment with the SLX produced a highly focused lesion running from cortex to medulla and often spanning the full thickness of the kidney. Unlike the diffuse interstitial haemorrhage observed with the HM3, the SLX lesion bore a blood-filled core of near-complete tissue disruption devoid of histologically recognizable kidney structure. • Despite the intensity of tissue destruction at the core of the lesion, measures of lesion size based on macroscopic determination of haemorrhage in the parenchyma were not significantly different from kidneys treated using the HM3 (2000 SWs, 120 SWs/min: SLX, 1.86 ± 0.52% FRV; HM3, 3.93 ± 1.29% FRV). • Doubling the SW dose of the SLX from 2000 to 4000 SWs did not significantly increase lesion size. In addition, slowing the firing rate of the SLX to 60 SWs/min did not reduce the size of the lesion (2.16 ± 0.96% FRV) compared with treatment at 120 SWs/min, as was the case with the HM3 (0.42 ± 0.23% FRV vs 3.93 ± 1.29% FRV). • Renal function fell significantly below baseline in all treated groups but was similar for both lithotriptors. • Focal width of the SLX (≈2.6 mm) was about one-third that of the HM3 (≈8 mm) while peak pressures were higher (SLX at power level 9: P+≈90 MPa, P-≈-12 MPa; HM3 at 24 kV: P+≈46 MPa, P-≈-8 MPa).
Conclusions: • The lesion produced by the SLX (narrow focal width, high acoustic pressure) was a more focused, more intense form of tissue damage than occurs with the HM3. • Slowing the SW rate to 60 SWs/min, a strategy shown to be effective in reducing injury with the HM3, was not protective with the SLX. • These findings suggest that the focal width and acoustic output of a lithotriptor affect the renal response to SWL.
© 2012 BJU INTERNATIONAL.
Figures
References
-
- Evan AP, Willis LR, Lingeman JE, McAteer JA. Renal trauma and the risk of long-term complications in shock wave lithotripsy. Nephron. 1998;78:1–8. - PubMed
-
- Connors BA, Evan AP, Willis LR, Blomgren PM, Lingeman JE, Fineberg NS. The effect of discharge voltage on renal injury and impairment caused by lithotripsy in the pig. J Am Soc Nephrol. 2000;11:310–8. - PubMed
-
- Lingeman J, Delius M, Evan A, Gupta M, Sarica K, Strohmaier W, McAteer J, Williams J. Bioeffects and physical mechanisms of SW effects in SWL. In: Segura J, Conort P, Khoury S, Pak C, Preminger GM, Tolley D, editors. Stone Disease: First International Consultation on Stone Disease. Heath Publications; Paris: 2003. pp. 251–286.
-
- Lingeman JE, Matlaga BR, Evan AP. Surgical management of upper urinary tract calculi. In: Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Campbell-Walsh Urology. 9. II. Philadelphia: Saunders; 2007. pp. 1431–507. Chapt 44.
-
- Evan AP, Willis LR. Extracorporeal shock wave lithotripsy: Complications. In: Smith AD, Badlani GH, Bagley DH, Clayman RV, Docimo SG, Jordan GH, Kavoussi LR, Lee BR, Lingeman JE, Preminger GM, Segura JW, editors. Smith’s Textbook on Endourology. Hamilton, Ontario, Canada: BC Decker, Inc; 2007. pp. 353–365.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
