

Reinfarction after percutaneous coronary intervention or medical management using the universal definition in patients with total occlusion after myocardial infarction: results from long-term follow-up of the Occluded Artery Trial (OAT) cohort
- PMID: 22520521
- PMCID: PMC4238915
- DOI: 10.1016/j.ahj.2012.01.016
Reinfarction after percutaneous coronary intervention or medical management using the universal definition in patients with total occlusion after myocardial infarction: results from long-term follow-up of the Occluded Artery Trial (OAT) cohort
Abstract
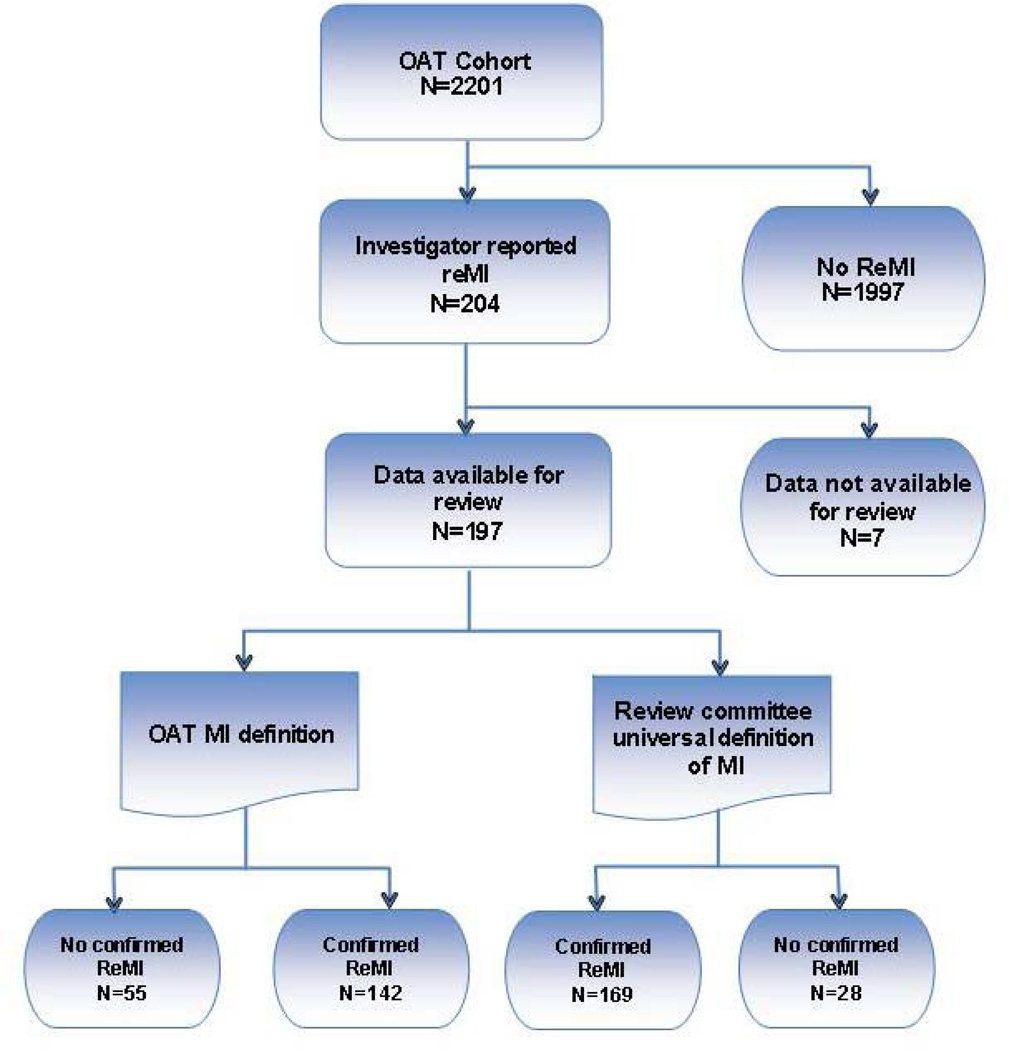
Background: The OAT study randomized 2,201 patients with a totally occluded infarct-related artery on days 3 to 28 (>24 hours) after myocardial infarction (MI) to percutaneous coronary intervention (PCI) or medical treatment (MED). There was no difference in the primary end point of death, reinfarction, or heart failure at 2.9 or 6-year mean follow-up. However, in patients randomized to PCI, there was a trend toward a higher rate of reinfarction.
Methods: We analyzed the characteristics and types of reinfarction according to the universal definition. Independent predictors of reinfarction were determined using Cox proportional hazard models with follow-up up to 9 years.
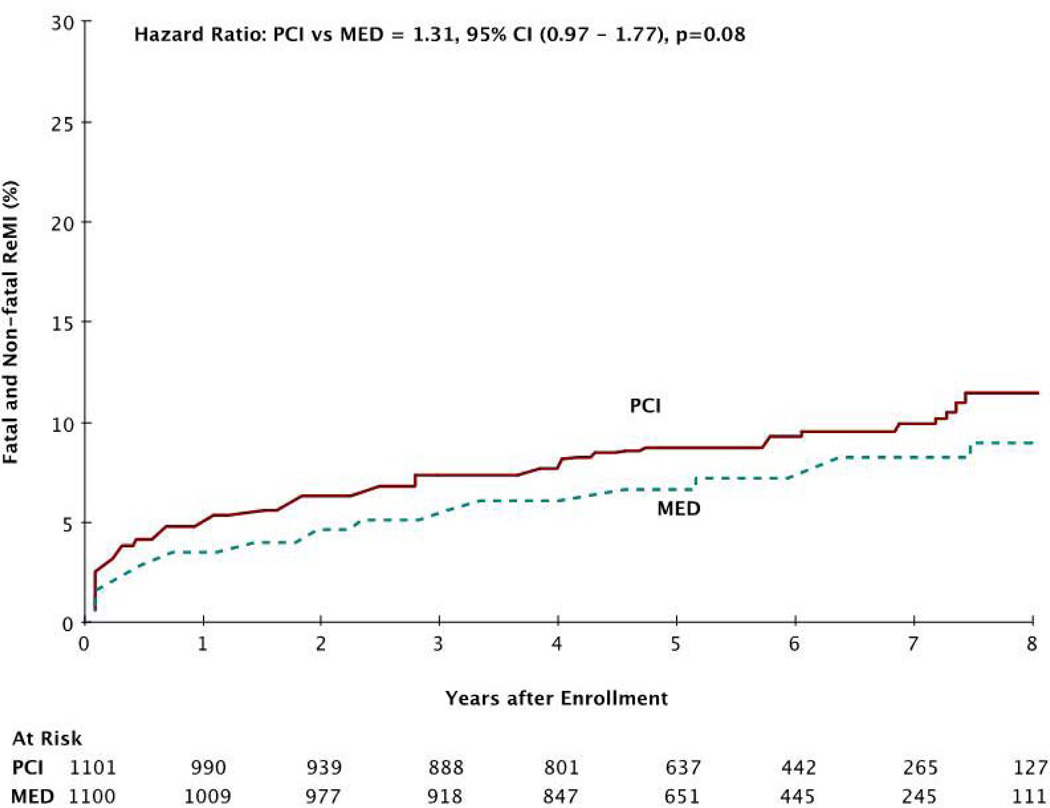
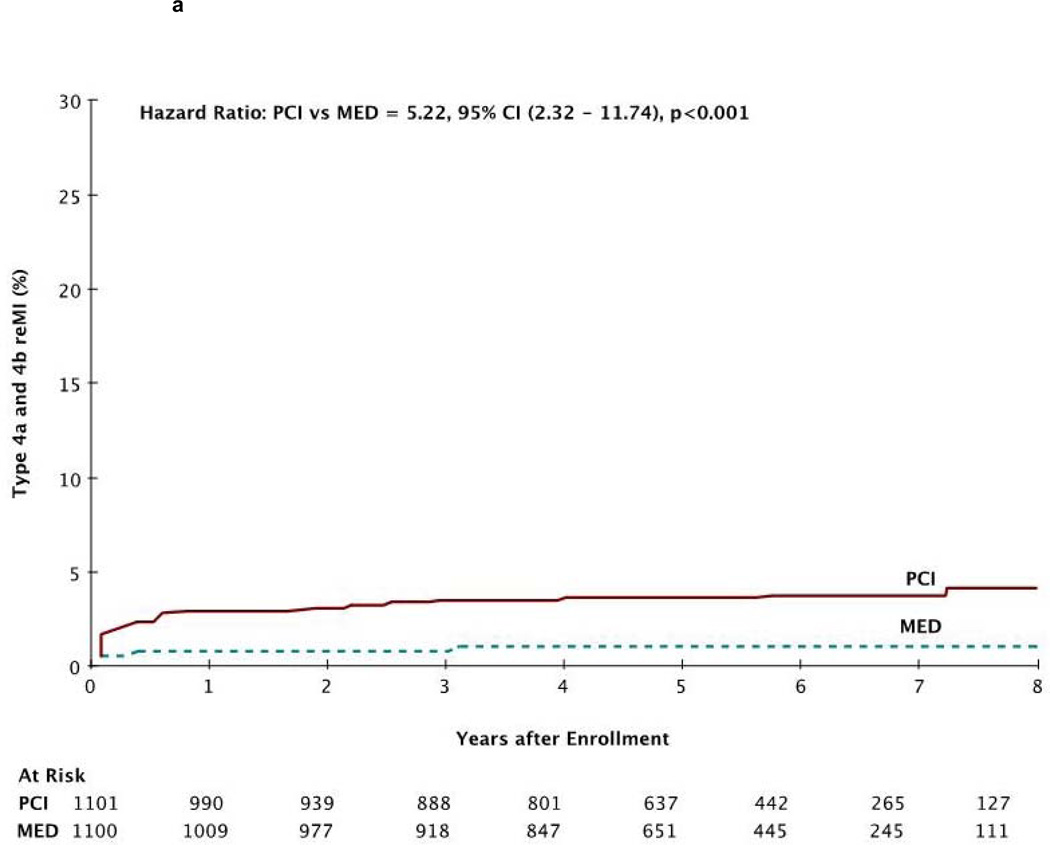
Results: There were 169 reinfarctions: 9.4% PCI vs 8.0% MED, hazard ratio 1.31, 95% CI 0.97-1.77, P = .08. Spontaneous reinfarction (type 1) occurred with similar frequency in the groups: 4.9% PCI vs 6.7% MED, hazard ratio 0.78, 95% CI 0.53-1.15, P = .21. Rates of type 2 (secondary) and 3 (sudden death) MI were similar in both groups. There was an increase in type 4a reinfarctions (related to protocol or other PCI) (0.8% PCI vs 0.1% MED, P = .01) and type 4b reinfarctions (stent thrombosis) (2.7% PCI vs 0.6% MED, P < .001). Multivariate predictors of reinfarction were history of PCI before study entry (P = .001), diabetes (P = .005), and absence of new Q waves with the index infarction (P = .01).
Conclusions: There was a trend for reinfarctions to be more frequent with PCI. Opening an occluded infarct-related artery in stable patients with late post-MI may expose them to a risk of subsequent reinfarction related to reocclusion and stent thrombosis.
Copyright © 2012 Mosby, Inc. All rights reserved.
Conflict of interest statement
Drs White, Reynolds, Carvalho, Liu, Martin, Pearte, Knatterud, Kruk, Cantor, Menon and Hochman report having no conflict of interest.
Figures

References
-
- Hochman JS, Lamas GA, Knatterud GL, et al. Design and methodology of the Occluded Artery Trial (OAT) Am Heart J. 2005;150:627–642. - PubMed
-
- Thygesen K, Alpert JS, White HD, et al. Universal definition of myocardial infarction. Circulation. 2007;116:2634–2653. - PubMed
-
- Hochman JS, Reynolds HR, Dzavik V, et al. Persistent lack of benefit of late revascularization of the occluded coronary artery post-MI - The Occluded Artery Trial (OAT) Long Term Results. Circulation. 2010;122:A13116.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
